Addictions
“Unscientific and bizarre”: Yet another Toronto addiction physician criticizes Canada’s “safer supply” experiment


By Liam Hunt
“It seems to be motivated by a very small, vocal, and well-connected group of advocates” says Dr. Michael Lester
Dr. Michael Lester, a Toronto-based addiction physician with 30 years of experience, says Canada’s “safer supply” programs are “inherently dangerous” and causing “dystopian” community harms due to widespread fraud.
These programs claim to reduce overdoses and deaths by distributing free addictive drugs—typically 8-milligram tablets of hydromorphone, an opioid as potent as heroin—to dissuade addicts from consuming riskier street substances. Yet experts across Canada say recipients regularly divert (sell or trade) their safer supply on the black market to acquire stronger illicit drugs, which then fuels addiction and organized crime.
“I have a couple dozen patients in my practice who were drug-free prior to the advent of safe supply, and they’ve gone back to using opioids in a destructive way because of the availability of diverted hydromorphone,” said Lester. “Every single day that I go to work, people tell me they’re struggling with the temptation not to take diverted safe supply. They don’t want to take it, but they take it anyway just because it’s cheap and available.”
After safer supply programs became widely accessible across Canada in 2020, Lester’s patients reported an influx of 8-milligram hydromorphone tablets on the black market, coinciding with a crash in the drug’s street price from $15–$20 per pill to just $2. He now estimates that 80 percent of his patients struggling with opioid addiction have relapsed due to diverted safer supply, leading some to abandon treatment entirely.
“Even if it’s sold at the rock-bottom price of $2 or $3 a pill, a person would make tens of thousands of dollars a year, which would have a tremendous impact on their ability to buy other drugs,” he explained. “Selling hydromorphone is too tempting not to do it, which keeps them entrenched in the whole world of dealing with opioid users and having opioids in their premises.”
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Lester said safer supply is evidently “fueling organized crime” because drug seizures in Ontario now commonly include hydromorphone, “which wasn’t happening before.” He added that some individuals who try these diverted drugs later transition to stronger opioids, such as fentanyl.
In July, for example, the London Police Service announced that seizures of hydromorphone had increased by more than 3,000 percent in the city since 2020. According to London Police Chief Thai Truong, “Diverted safer supply is being resold into our community. There’s organized drug trafficking at the highest levels of organized crime, and there’s drug trafficking at the street level. We’re seeing all of it.”
While Lester acknowledges that safer supply can be useful as a “treatment of last resort, after traditional treatments have been tried and failed,” he said it is now being offered immediately to a wide variety of patients, which has “decimated” uptake of traditional addiction therapies, such as methadone and Suboxone.
As a result, conventional addiction clinics are now at risk of shutting down, meaning some communities could lose access to gold-standard treatments (i.e., methadone and Suboxone) while highly profitable, but unscientific, safer supply programs take over instead.
Lester said the evidence supporting safer supply is biased and “misleading” because, generally speaking, these studies simply interview enrolled patients and ask them to self-report whether they benefit from the programs. He noted that many safer supply researchers are public health academics, not doctors, meaning they lack clinical experience with the communities they study.
“It seems to be motivated by a very small, vocal, and well-connected group of advocates that has completely changed the landscape in addiction medicine treatment in a very short time,” he said.
Lester argues that some safer supply researchers seem to purposefully design their study methodologies to favor the programs and disregard systemic harms. He said this flawed science is then propagated by credulous journalists who fail to adequately scrutinize agenda-driven research.
While he personally knows “a couple dozen” colleagues in addiction medicine who regularly express skepticism about safer supply, many have been reluctant to speak out, fearing backlash from activist groups that “terrorize” critics.
“The stories are common of people being harassed and insulted on social media. We’ve heard of doctors being threatened [and] dropped from committees because they spoke out.”
For example, after Lester and his colleagues published two open letters criticizing safer supply in late 2023, they were targeted by a series of articles by Drug Data Decoded, a popular Canadian harm reduction Substack, which compared the doctors to Nazis and eugenicists. The articles were then widely shared on social media by safer supply activists.
Lester recalled an incident in which harm reduction activists targeted a doctor’s daughter at her high school in retaliation for her parent’s public criticism of safer supply.
“It’s just something that seems so unscientific and so bizarre in medicine,” he said. “Physicians just aren’t used to a powerful political lobby changing a treatment protocol.”
After Lester and more than a dozen of his colleagues wrote several public letters calling for reform and requested a meeting with Ya’ara Saks, the federal Minister of Mental Health and Addictions, they found themselves “sidelined and ignored.”
After months of delays, they were able to present their clinical observations to Saks, only to have her disregard them and incorrectly claim, weeks later, that criticism of safer supply is rooted in “fear and stigma.”
“The insults aren’t a big enough consequence to keep me from speaking my mind,” he declared.
After a short reflection, he then added, “If anyone doesn’t have a stigma against this population, it’s me. I’ve dedicated my life to helping them.”
Liam Hunt is a Canadian writer and journalist with an interest in humanism, international affairs, and crime and justice. This story is produced by the Centre For Responsible Drug Policy’s “Experts Speak Up” series in partnership with the Macdonald-Laurier Institute.
Our content is always free – but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.
2025 Federal Election
Study links B.C.’s drug policies to more overdoses, but researchers urge caution
By Alexandra Keeler
A study links B.C.’s safer supply and decriminalization to more opioid hospitalizations, but experts note its limitations
A new study says B.C.’s safer supply and decriminalization policies may have failed to reduce overdoses. Furthermore, the very policies designed to help drug users may have actually increased hospitalizations.
“Neither the safer opioid supply policy nor the decriminalization of drug possession appeared to mitigate the opioid crisis, and both were associated with an increase in opioid overdose hospitalizations,” the study says.
The study has sparked debate, with some pointing to it as proof that B.C.’s drug policies failed. Others have questioned the study’s methodology and conclusions.
“The question we want to know the answer to [but cannot] is how many opioid hospitalizations would have occurred had the policy not have been implemented,” said Michael Wallace, a biostatistician and associate professor at the University of Waterloo.
“We can never come up with truly definitive conclusions in cases such as this, no matter what data we have, short of being able to magically duplicate B.C.”
Jumping to conclusions
B.C.’s controversial safer supply policies provide drug users with prescription opioids as an alternative to toxic street drugs. Its decriminalization policy permitted drug users to possess otherwise illegal substances for personal use.
The peer-reviewed study was led by health economist Hai Nguyen and conducted by researchers from Memorial University in Newfoundland, the University of Manitoba and Weill Cornell Medicine, a medical school in New York City. It was published in the medical journal JAMA Health Forum on March 21.
The researchers used a statistical method to create a “synthetic” comparison group, since there is no ideal control group. The researchers then compared B.C. to other provinces to assess the impact of certain drug policies.
Examining data from 2016 to 2023, the study links B.C.’s safer supply policies to a 33 per cent rise in opioid hospitalizations.
The study says the province’s decriminalization policies further drove up hospitalizations by 58 per cent.
“Neither the safer supply policy nor the subsequent decriminalization of drug possession appeared to alleviate the opioid crisis,” the study concludes. “Instead, both were associated with an increase in opioid overdose hospitalizations.”
The B.C. government rolled back decriminalization in April 2024 in response to widespread concerns over public drug use. This February, the province also officially acknowledged that diversion of safer supply drugs does occur.
The study did not conclusively determine whether the increase in hospital visits was due to diverted safer supply opioids, the toxic illicit supply, or other factors.
“There was insufficient evidence to conclusively attribute an increase in opioid overdose deaths to these policy changes,” the study says.
Nguyen’s team had published an earlier, 2024 study in JAMA Internal Medicine that also linked safer supply to increased hospitalizations. However, it failed to control for key confounders such as employment rates and naloxone access. Their 2025 study better accounts for these variables using the synthetic comparison group method.
The study’s authors did not respond to Canadian Affairs’ requests for comment.
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Correlation vs. causation
Chris Perlman, a health data and addiction expert at the University of Waterloo, says more studies are needed.
He believes the findings are weak, as they show correlation but not causation.
“The study provides a small signal that the rates of hospitalization have changed, but I wouldn’t conclude that it can be solely attributed to the safer supply and decrim[inalization] policy decisions,” said Perlman.
He also noted the rise in hospitalizations doesn’t necessarily mean more overdoses. Rather, more people may be reaching hospitals in time for treatment.
“Given that the [overdose] rate may have gone down, I wonder if we’re simply seeing an effect where more persons survive an overdose and actually receive treatment in hospital where they would have died in the pre-policy time period,” he said.
The Nguyen study acknowledges this possibility.
“The observed increase in opioid hospitalizations, without a corresponding increase in opioid deaths, may reflect greater willingness to seek medical assistance because decriminalization could reduce the stigma associated with drug use,” it says.
“However, it is also possible that reduced stigma and removal of criminal penalties facilitated the diversion of safer opioids, contributing to increased hospitalizations.”
Karen Urbanoski, an associate professor in the Public Health and Social Policy department at the University of Victoria, is more critical.
“The [study’s] findings do not warrant the conclusion that these policies are causally associated with increased hospitalization or overdose,” said Urbanoski, who also holds the Canada Research Chair in Substance Use, Addictions and Health Services.
Her team published a study in November 2023 that measured safer supply’s impact on mortality and acute care visits. It found safer supply opioids did reduce overdose deaths.
Critics, however, raised concerns that her study misrepresented its underlying data and showed no statistically significant reduction in deaths after accounting for confounding factors.
The Nguyen study differs from Urbanoski’s. While Urbanoski’s team focused on individual-level outcomes, the Nguyen study analyzed broader, population-level effects, including diversion.
Wallace, the biostatistician, agrees more individual-level data could strengthen analysis, but does not believe it undermines the study’s conclusions. Wallace thinks the researchers did their best with the available data they had.
“We do not have a ‘copy’ of B.C. where the policies weren’t implemented to compare with,” said Wallace.
B.C.’s overdose rate of 775 per 100,000 is well above the national average of 533.
Elenore Sturko, a Conservative MLA for Surrey-Cloverdale, has been a vocal critic of B.C.’s decriminalization and safer supply policies.
“If the government doesn’t want to believe this study, well then I invite them to do a similar study,” she told reporters on March 27.
“Show us the evidence that they have failed to show us since 2020,” she added, referring to the year B.C. implemented safer supply.
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Our content is always free – but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.

By Alexandra Keeler
The move follows explosive revelations that more than 60 B.C. pharmacies were allegedly participating in a scheme to overbill the government under its safer supply program. The scheme involved pharmacies incentivizing clients to fill prescriptions they did not require by offering them cash or rewards. Some of those clients then sold the drugs on the black market.
An addiction medicine advocacy group is urging B.C. to promptly issue new guidelines for witnessed dosing of drugs dispensed under the province’s controversial safer supply program.
In a March 24 letter to B.C.’s health minister, Addiction Medicine Canada criticized the BC Centre on Substance Use for dragging its feet on delivering the guidelines and downplaying the harms of prescription opioids.
The centre, a government-funded research hub, was tasked by the B.C. government with developing the guidelines after B.C. pledged in February to return to witnessed dosing. The government’s promise followed revelations that many B.C. pharmacies were exploiting rules permitting patients to take safer supply opioids home with them, leading to abuse of the program.
“I think this is just a delay,” said Dr. Jenny Melamed, a Surrey-based family physician and addiction specialist who signed the Addiction Medicine Canada letter. But she urged the centre to act promptly to release new guidelines.
“We’re doing harm and we cannot just leave people where they are.”
Addiction Medicine Canada’s letter also includes recommendations for moving clients off addictive opioids altogether.
“We should go back to evidence-based medicine, where we have medications that work for people in addiction,” said Melamed.
‘Best for patients’
On Feb. 19, the B.C. government said it would return to a witnessed dosing model. This model — which had been in place prior to the pandemic — will require safer supply participants to take prescribed opioids under the supervision of health-care professionals.
The move follows explosive revelations that more than 60 B.C. pharmacies were allegedly participating in a scheme to overbill the government under its safer supply program. The scheme involved pharmacies incentivizing clients to fill prescriptions they did not require by offering them cash or rewards. Some of those clients then sold the drugs on the black market.
In its Feb. 19 announcement, the province said new participants in the safer supply program would immediately be subject to the witnessed dosing requirement. For existing clients of the program, new guidelines would be forthcoming.
“The Ministry will work with the BC Centre on Substance Use to rapidly develop clinical guidelines to support prescribers that also takes into account what’s best for patients and their safety,” Kendra Wong, a spokesperson for B.C.’s health ministry, told Canadian Affairs in an emailed statement on Feb. 27.
More than a month later, addiction specialists are still waiting.
According to Addiction Medicine Canada’s letter, the BC Centre on Substance Use posed “fundamental questions” to the B.C. government, potentially causing the delay.
“We’re stuck in a place where the government publicly has said it’s told BCCSU to make guidance, and BCCSU has said it’s waiting for government to tell them what to do,” Melamed told Canadian Affairs.
This lag has frustrated addiction specialists, who argue the lack of clear guidance is impeding the transition to witnessed dosing and jeopardizing patient care. They warn that permitting take-home drugs leads to more diversion onto the streets, putting individuals at greater risk.
“Diversion of prescribed alternatives expands the number of people using opioids, and dying from hydromorphone and fentanyl use,” reads the letter, which was also co-signed by Dr. Robert Cooper and Dr. Michael Lester. The doctors are founding board members of Addiction Medicine Canada, a nonprofit that advises on addiction medicine and advocates for research-based treatment options.
“We have had people come in [to our clinic] and say they’ve accessed hydromorphone on the street and now they would like us to continue [prescribing] it,” Melamed told Canadian Affairs.
A spokesperson for the BC Centre on Substance Use declined to comment, referring Canadian Affairs to the Ministry of Health. The ministry was unable to provide comment by the publication deadline.
Big challenges
Under the witnessed dosing model, doctors, nurses and pharmacists will oversee consumption of opioids such as hydromorphone, methadone and morphine in clinics or pharmacies.
The shift back to witnessed dosing will place significant demands on pharmacists and patients. In April 2024, an estimated 4,400 people participated in B.C.’s safer supply program.
Chris Chiew, vice president of pharmacy and health-care innovation at the pharmacy chain London Drugs, told Canadian Affairs that the chain’s pharmacists will supervise consumption in semi-private booths.
Nathan Wong, a B.C.-based pharmacist who left the profession in 2024, fears witnessed dosing will overwhelm already overburdened pharmacists, creating new barriers to care.
“One of the biggest challenges of the retail pharmacy model is that there is a tension between making commercial profit, and being able to spend the necessary time with the patient to do a good and thorough job,” he said.
“Pharmacists often feel rushed to check prescriptions, and may not have the time to perform detailed patient counselling.”
Others say the return to witnessed dosing could create serious challenges for individuals who do not live close to health-care providers.
Shelley Singer, a resident of Cowichan Bay, B.C., on Vancouver Island, says it was difficult to make multiple, daily visits to a pharmacy each day when her daughter was placed on witnessed dosing years ago.
“It was ridiculous,” said Singer, whose local pharmacy is a 15-minute drive from her home. As a retiree, she was able to drive her daughter to the pharmacy twice a day for her doses. But she worries about patients who do not have that kind of support.
“I don’t believe witnessed supply is the way to go,” said Singer, who credits safer supply with saving her daughter’s life.
Melamed notes that not all safer supply medications require witnessed dosing.
“Methadone is under witness dosing because you start low and go slow, and then it’s based on a contingency management program,” she said. “When the urine shows evidence of no other drug, when the person is stable, [they can] take it at home.”
She also noted that Suboxone, a daily medication that prevents opioid highs, reduces cravings and alleviates withdrawal, does not require strict supervision.
Kendra Wong, of the B.C. health ministry, told Canadian Affairs that long-acting medications such as methadone and buprenorphine could be reintroduced to help reduce the strain on health-care professionals and patients.
“There are medications available through the [safer supply] program that have to be taken less often than others — some as far apart as every two to three days,” said Wong.
“Clinicians may choose to transition patients to those medications so that they have to come in less regularly.”
Such an approach would align with Addiction Medicine Canada’s recommendations to the ministry.
The group says it supports supervised dosing of hydromorphone as a short-term solution to prevent diversion. But Melamed said the long-term goal of any addiction treatment program should be to reduce users’ reliance on opioids.
The group recommends combining safer supply hydromorphone with opioid agonist therapies. These therapies use controlled medications to reduce withdrawal symptoms, cravings and some of the risks associated with addiction.
They also recommend limiting unsupervised hydromorphone to a maximum of five 8 mg tablets a day — down from the 30 tablets currently permitted with take-home supplies. And they recommend that doses be tapered over time.
“This protocol is being used with success by clinicians in B.C. and elsewhere,” the letter says.
“Please ensure that the administrative delay of the implementation of your new policy is not used to continue to harm the public.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle


The Federal Brief That Should Sink Carney
How Canada’s Mainstream Media Lost the Public Trust

Ottawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
Real Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
2025 Federal Election10 hours ago
The Federal Brief That Should Sink Carney
-
2025 Federal Election12 hours ago
How Canada’s Mainstream Media Lost the Public Trust
-
2025 Federal Election15 hours ago
Ottawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
2025 Federal Election14 hours ago
Real Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
 John Stossel11 hours ago
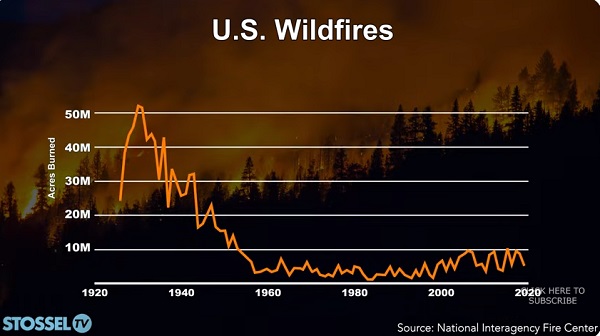
John Stossel11 hours agoClimate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
 COVID-1913 hours ago
COVID-1913 hours agoNearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal
-
 Entertainment2 days ago
Entertainment2 days agoPedro Pascal launches attack on J.K. Rowling over biological sex views
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoPoilievre Campaigning To Build A Canadian Economic Fortress