Health
UK’s NHS set to launch detransitioning services for ‘transgender’ patients


From LifeSiteNews
A report showing that clinical practice for ‘transgenders’ is built on ‘shaky foundations’ prompted the UK’s Health Service to work toward ‘detransitioning’ services.
The National Health Service of England (NHS) is slated to launch its first “detransitioning” service aimed at returning “transgender” individuals to physical conformity with their biological sex.
The move was prompted by the recommendations of a review of Gender Identity Services by pediatrician Dr. Hilary Cass, The Telegraph reported. Dr. Cass’ report found an “exponential” spike in the number of young people who were presented to the UK NHS Gender Identity Service (GIDS) beginning in 2014.
General Practitioners in England were found to be “pressurized to prescribe hormones” by patients who had not consulted with a private clinician, and Dr. Cass concluded that the current practice of so-called “gender medicine” in the U.K., involving the use of puberty blockers and cross-sex hormones, was built on “shaky foundations.”
Dr. Cass reportedly went so far as to recommend that GPs resist efforts by private practitioners to prescribe puberty blockers and cross-sex hormones, “particularly if that private provider is acting outside NHS guidance.”
NHS England has decided to fully adopt Dr. Cass’ recommendations, and on Wednesday published its plans to reform its gender services accordingly. Sir Stephen Prowis, medical director of the NHS, praised Dr. Cass’ work as “invaluable” and said the NHS would now embrace a “fundamentally different and safer model of care for children.”
According to Health Service officials, the NHS’ next step is to “define” a “pathway” for those who decide to detransition, since there is currently no official guidance on how to care for such individuals. Their work will involve examining the proportion of patients who detransition, and their reasons for detransitioning, The Telegraph reported.
The plan involves the creation of six new clinics by 2026 specialized to care for minors struggling with their biological sex.

Despite this impending reform, the NHS is set to begin clinical trials of puberty blockers for minors, since Dr. Cass’ report cited lack of long-term studies as a reason that puberty blockers should not be prescribed to minors.
Critics have warned that these trials are “ethically unjustifiable,” with the warning that they “pose the very real risk of the NHS sacrificing the otherwise good health of vulnerable children and causing them grave physical harm in the name of research.”
Lucy Marsh of the Family Education Trust has called upon the NHS to address the roots of gender dysphoria and has decried its planned trials of administering puberty blockers to teenagers as “unethical” and “dangerous.”
‘We do not need more gender clinics, instead the NHS should be looking at the root causes of gender dysphoria including mental health issues, autism, sexual abuse and issues within the family,” said Marsh, according to The Daily Mail.
“It is not ‘kind’ to lead children down a pathway that leads to irreversible harm and destroys families,” she said, adding that it is a “a huge waste of taxpayer’s money to roll out gender clinics to every area of England.”
Transgender hormonal and surgical interventions are known to cause lifelong mental and physical damage and to exacerbate psychological issues in those subjected to them.
Studies find that more than 80 percent of children experiencing gender dysphoria outgrow it on their own by late adolescence, and that even full “reassignment” surgery often fails to resolve gender-confused individuals’ heightened tendency to engage in self-harm and suicide – and may even exacerbate it, including by reinforcing their confusion and neglecting the actual root causes of their mental strife.
Many oft-ignored detransitioners have attested to the physical and mental harm of reinforcing gender confusion as well as to the bias and negligence of the medical establishment on the subject, many of whom take an activist approach to their profession and begin cases with a predetermined conclusion that “transitioning” is the best solution.


ACIP voted to un-recommend the Hep B birth dose, but here’s the problem: they still can’t weigh the other side of the ledger
Sunday, something happened that has never happened in the history of American public health: ACIP voted 8-3 to un-recommend the universal birth dose of hepatitis B for babies born to mothers who test negative for the virus. After 34 years of jabbing every American newborn within hours of taking their first breath—regardless of whether their mother had hepatitis B—the committee finally acknowledged what 25 European countries figured out decades ago: it doesn’t make sense.
But watching this vote unfold, I couldn’t help but notice the absurdity of the debate itself. Committee members who opposed the change kept saying variations of the same thing: “We’ve heard ‘do no harm’ as a moral imperative. We are doing harm by changing this wording.” Another said “no rational science has been presented” to support the change.
How to End the Autism Epidemic is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
And therein lies the fundamental problem with ACIP—and with the entire vaccine regulatory apparatus in America. They literally cannot weigh risk versus benefit because they only have data on one side of the scale.
The Missing Side of the Ledger
When ACIP debates adding or removing a vaccine from the schedule, they can produce endless data on disease incidence. They can show you charts demonstrating how hepatitis B cases in infants dropped from thousands to single digits after 1991. They can model projected infections if vaccination rates decline. They have this data at their fingertips because tracking infectious disease is something our public health apparatus actually does.
But ask them to produce equivalent data on vaccine injury, and you’ll get silence. Not “the data shows injuries are rare.” Not “here’s our comprehensive tracking of adverse events.” Just… nothing. A void where information should be.
This is not an accident. This is by design.
The safety trials for Engerix-B and Recombivax HB—the two hepatitis B vaccines given to American newborns—monitored adverse events for four to five days after injection. That’s it. If your baby developed seizures on day six, or regressed into autism over the following months, or developed autoimmune disease in the following year—none of that would appear in the pre-licensure safety data.
And the post-market surveillance? VAERS is a voluntary reporting system that the CDC itself acknowledges captures only a tiny fraction of adverse events. A Harvard-funded study found it captures perhaps 1% of actual vaccine injuries. Vaccine court has paid out over $5 billion in claims while simultaneously being structured to make filing nearly impossible for average families.
So when Dr. Cody Meissner voted against removing the Hep B birth dose and said he saw “clear evidence of the benefits” but “not the harms,” he was accidentally revealing the entire rotten structure. Of course he doesn’t see the harms. Nobody is systematically looking for them.
The Invisibility of Vaccine Injury
Here’s what most people don’t understand about vaccine injury: it’s nothing like a gunshot wound.
If you shoot someone, the cause is obvious. There’s a bullet, a wound, blood, a clear mechanism of action visible to any observer. Even a medical examiner who’s never seen the victim before can determine cause of death.
Vaccine injury doesn’t work that way. When aluminum nanoparticles from a vaccine cross the blood-brain barrier via macrophages, when they lodge in brain tissue and trigger chronic neuroinflammation, when a child slowly regresses over weeks or months—there’s no bullet. There’s no smoking gun. There’s just a before and an after, and a desperate parent trying to explain to doctors that something changed.
This invisibility is the vaccine program’s greatest protection. Because the injury mechanism is complex and delayed, because it doesn’t leave an obvious wound, because it requires actually looking to find—and because no one in authority is looking—the injuries simply don’t exist in the official record.
I watched my own son Jamie regress after his vaccines. A healthy, developing toddler who lost his words, stopped making eye contact, and retreated into a world we couldn’t reach. My wife and I know what happened. Thousands of other parents know the same thing happened to their children. But because this type of injury doesn’t show up on a simple blood test, because there’s no autopsy finding that says “vaccine-induced encephalopathy,” ACIP members can sit in a room and say with straight faces that they don’t see evidence of harm.
They’re not lying. They literally can’t see it. Because no one is measuring it.
The Chicken Pox Conundrum
Here’s an example that illustrates the insanity of our current approach.
The varicella (chicken pox) vaccine was added to the schedule in 1995. It definitely reduces chicken pox cases. The data is clear on that front. Mission accomplished, right?
But what about the other side of the ledger?
Emerging research suggests that wild chicken pox infection provides some protective effect against brain cancers—particularly glioma, the most common type of primary brain tumor. Multiple studies have found that people who had chicken pox as children have significantly lower rates of brain cancer later in life. The hypothesis is that the immune response to wild varicella provides lasting immunological benefits that extend far beyond preventing itchy spots.
Meanwhile, the vaccine itself has been associated with increased rates of autoimmune conditions. Studies have linked varicella vaccination to higher rates of herpes zoster (shingles) outbreaks in younger age groups, to autoimmune disorders, to various adverse events that weren’t captured in the original short-term safety trials.
So what’s the true risk-benefit of the chicken pox vaccine? Does preventing a week of itchy discomfort in childhood justify potentially increased rates of brain cancer and autoimmune disease later in life?
ACIP can’t answer this question. They literally don’t have the data. They can show you chicken pox cases going down. They cannot show you a comprehensive analysis of long-term neurological and immunological outcomes in vaccinated versus unvaccinated populations, because that study has never been done.
And so they keep recommending the vaccine based on the only data they have—the disease prevention data—while remaining willfully blind to consequences they’ve never bothered to measure.
The ACIP Paradox
Sunday’s vote was historic, but it also revealed the fundamental paradox of vaccine regulation in America.
The committee members who voted to remove the universal Hep B birth dose recommendation did so largely based on comparative evidence from Europe, parental concerns, and the basic logic that vaccinating a 12-hour-old baby for a sexually transmitted disease their mother doesn’t have makes no medical sense. They were right to do so.
But the committee members who voted against the change weren’t wrong either, from their perspective. They looked at the only data they have—disease prevention data—and concluded that removing the recommendation could lead to more hepatitis B cases. And within their limited framework, they’re correct.
The problem is the framework itself.
True risk-benefit analysis requires data on both risks AND benefits. ACIP has comprehensive data on benefits (disease prevention) and virtually no data on risks (vaccine injury). So every decision they make is fundamentally flawed from the start.
When Dr. Joseph Hibbeln complained that “no rational science has been presented” to support changing the recommendations, he was inadvertently indicting the entire system. Of course no comprehensive vaccine injury data was presented—such data doesn’t exist because no one has been willing to collect it.
This is like asking someone to make an informed financial decision while only showing them potential profits and hiding all possible losses. Of course the decision will be skewed. Of course you’ll end up with a bloated portfolio of high-risk investments that look great on paper.
The Real Reform
If RFK Jr. and the new HHS leadership want to actually fix the vaccine program, they need to understand that removing individual vaccines or making them “optional” is just rearranging deck chairs on the Titanic.
The real reform is creating the data infrastructure that should have existed from the beginning.
We need a comprehensive, long-term, vaccinated-versus-unvaccinated health outcomes study. Not a five-day safety trial. A multi-decade tracking of neurological, immunological, and developmental outcomes across populations with varying vaccination status. Florida just eliminated all vaccine mandates—that state alone could provide the data we need within ten years if someone had the courage to actually collect it.
We need a vaccine injury surveillance system that actually captures adverse events. Not a voluntary reporting system that misses 99% of injuries. An active surveillance system with trained clinicians looking for the kinds of delayed, complex injuries that vaccines actually cause.
We need accountability for manufacturers. The 1986 National Childhood Vaccine Injury Act removed all liability from vaccine makers—and predictably, the vaccine schedule exploded afterward while safety research stagnated. Why would any company invest in safety when they can’t be sued for injuries?
Without this data, every ACIP meeting will be the same performance we watched this week: members confidently citing disease prevention data while admitting they can’t see evidence of harm—not because harm doesn’t exist, but because no one is looking for it.
What Comes Next
Sunday’s vote was a crack in the wall. For the first time, an American regulatory body acknowledged that perhaps vaccinating every newborn within hours of birth for a disease primarily transmitted through sex and IV drug use doesn’t make sense when the mother has already tested negative.
But the forces of institutional inertia are already mobilizing. The American Academy of Pediatrics is “disappointed.” The American Medical Association is calling for the CDC to reject the recommendation. The pharmaceutical industry—which collects over $225 million annually from Hep B birth doses alone—will fight to restore the universal recommendation.
They will cite the same data they always cite: disease prevention data. Cases prevented. Infections avoided. Lives saved—theoretically.
They will not cite vaccine injury data, because that data doesn’t exist in any comprehensive form. They will not present long-term health outcomes in vaccinated versus unvaccinated children, because those studies have been actively avoided for decades. They will not acknowledge the thousands of families who have watched their children regress after vaccination, because those injuries aren’t captured in any official database.
And this is why ACIP will always be hamstrung. Until we build the data infrastructure to actually measure vaccine injury—to put real numbers on the other side of the ledger—every vaccine decision will be based on incomplete information. Every “risk-benefit analysis” will be a fraud, because we’re only measuring half the equation.
The hepatitis B birth dose vote was a small victory. But the larger battle—for actual science, for complete data, for true informed consent—that battle is just beginning.
And until we win it, ACIP will continue making decisions in the dark, confidently citing evidence of benefits while remaining deliberately blind to the harms they’ve never bothered to measure.
About the author
 |
J.B. Handley is the proud father of a child with Autism. He spent his career in the private equity industry and received his undergraduate degree with honors from Stanford University. His first book, How to End the Autism Epidemic, was published in September 2018. The book has sold more than 75,000 copies, was an NPD Bookscan and Publisher’s Weekly Bestseller, broke the Top 40 on Amazon, and has more than 1,000 Five-star reviews. Mr. Handley and his nonspeaking son are also the authors of Underestimated: An Autism Miracle and co-produced the film SPELLERS, available now on YouTube.
How to End the Autism Epidemic is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.


“While I question whether any baby should receive a vaccine against a rare disease in infancy, I am pleased that this is now a matter for parents and their healthcare practitioner to decide — not a state mandate based on a federal pharma-backed recommendation.”
Advisers to the Centers for Disease Control and Prevention (CDC) have voted to end a decades-long recommendation that all infants born in the U.S. receive the hepatitis B vaccine (Hep B) within 12-24 hours of birth.
Instead, for babies born to mothers who test negative for hepatitis B, the committee recommends that families determine whether to give their child the Hep B shot at birth through individual decision-making with their physician.
For infants who don’t get the birth dose, the committee recommends the initial dose of the vaccine not be administered until infants are at least 2 months old.
Three of the 11 committee members — Dr. Raymond Pollack, Dr. Cody Meissner and Dr. Joseph R. Hibbeln — opposed the recommendation. The remaining eight members supported it.
Andrew Johnson from the Centers for Medicare & Medicaid Services assured the committee that the language change will not affect Medicaid or insurance coverage of the vaccine.
For mothers whose hepatitis B status is unknown or who test positive, the birth dose recommendation remains in place.
Children’s Health Defense CEO Mary Holland, a long-time critic of the universal birth dose policy, welcomed the committee’s vote to “end the ill-considered universal recommendation for the Hep B birth vaccine dose.”
Holland added:
“The science behind that universal recommendation was a sham, based on thoroughly inadequate clinical trials. Hundreds of babies unquestionably died because of it. While I question whether any baby should receive a vaccine against a rare disease in infancy, I am pleased that this is now a matter for parents and their healthcare practitioner to decide — not a state mandate based on a federal pharma-backed recommendation.
“And while the ACIP [Advisory Committee on Immunization Practices] debate on this issue was tedious and rancorous at times, it is an extremely positive change that actual debate about childhood vaccines is occurring in government venues with impact. This is the transparency that Secretary Kennedy promised.”
Dr. Monique Yohanan, senior fellow for health policy at Independent Women, told The Defender there was never “a good science-based reason to have a universal vaccination that 99% of babies born in the United States are not at any risk,” and that the vote was “good news for babies.”
She added that she hoped it would “provide an opportunity to actually have outreach to the moms who are positive for hepatitis B, women who are immigrants, women who are IV drug users.” She said the previous policy was “performative compassion. And these are really underserved women who we ignored the outreach that they needed.”
The committee also voted 6-4 with one abstention that after the initial Hep B shot, parents should consult with healthcare providers to consider whether their child should have a serology test, which would show whether they had antibodies considered sufficient to protect them against the disease.
The committee voted to update the CDC Vaccines for Children (VFC) Program funding to match ACIP’s recommendations. Several committee members, including Meissner and Hibbeln, abstained from voting on the VFC resolution, protesting that they didn’t understand the implications of the vote — reflecting some of the disagreement that pervaded the two-day meeting.
The votes on the Hep B vaccine were originally scheduled for the September meeting, but were deferred to allow the CDC work group to put together more data to inform the committee’s decision.
Sunday’s vote was postponed from Saturday so members could have more time to review the language of the proposal.
Like flying in a plane that wasn’t safety tested?
The decision to postpone followed a contentious day-long meeting on Thursday, during which some members of the committee and liaisons from professional associations argued there was no need to change the recommendation, because there was no “evidence of harm” from the vaccine.
Advocates for changing the recommendation pointed to a near-complete lack of safety data — small clinical trials for the vaccines tracked infants for a week or less after the shot and little follow-up research on autoimmune and neurological disorders.
Big differences of opinion persisted at Sunday’s meeting.
ACIP member Retsef Levi, Ph.D., said that for parents whose children were at extremely low risk, the decision to give them the vaccine was analogous to flying in a plane — they wouldn’t get in a plane that hadn’t been safety tested, why should they give their child a vaccine that hadn’t been safety tested.
Meissner disagreed, saying, “We know vaccines are safe. There is no question that the COVID vaccine recommendations were dishonest, disingenuous, but the hepatitis B vaccine is very well established.”
In opening remarks, Dr. Robert Malone — who chaired the meeting because the newly named committee chairperson, Dr. Kirk Milhoun, is traveling — said “the credibility of the ACIP rests not on speed, but on rigor.”
Commenting on the heated discussions during Thursday’s meeting, Milhoun said that scientific debates are necessarily contentious.
“If they are not contentious, if they are not approached with rigor, then we end up with bad decisions. We end up with bad science. We must actively engage in responsible debate concerning contentious issues. We must boldly address change, risk new ideas, and conflicting hypotheses, which is the proper nature of evidence-based science.”
Dr. Jason Goldman, a liaison to the ACIP for the American College of Physicians, attacked opposing viewpoints as unscientific. Goldman said the Hep B vaccine discussion was “an unnecessary solution looking for a problem.”
‘If adults won’t go for the shots, then give them to babies’
The Hep B vaccine has been universally recommended for infants since 1991. The first shot is currently given within 24 hours after birth to prevent infection with hepatitis B from mothers who carry the disease — less than 0.5% of mothers.
Mothers can be tested in the hospital to determine whether they have the disease, and current tests have a 100% accuracy rate, according to FDA ex officio ACIP participant Tracy Beth Høeg, M.D., Ph.D.
However, a 1991 New York Times article posted on Substack yesterday by Dr. Meryl Nass showed that when the universal shot was rolled out, the goal was not to prevent maternal transmission — the goal was to prevent adult cases, at a time when adult cases were deemed a national crisis. However, adults commonly didn’t get the shot.
“If adults won’t go for the shots, then give them to babies,” the article said.
Following Thursday’s meeting, legacy media attacked the committee and the CDC’s presenters and highlighted charges of misinformation by liaison members. Liaisons are nonvoting members from professional medical organizations who can offer their opinions and advice to the committee.
Representatives from some of those groups, including the American Academy of Pediatrics (AAP) and the American Medical Association, were disinvited in August from participation in the workgroups due to conflicts of interest.
Since then, the AAP has boycotted the ACIP meetings
At the start of today’s meeting, Meissner castigated AAP for this move. He said he was concerned that by not participating, they would be seen as being more focused on making a political statement than attending to the health of children.
He said that pediatricians should be part of the discussions. “Refusal to participate in the ACIP meetings does not appear to be in the best interest of children.”
Immediately following today’s vote, the Times quoted “experts” from some of the staunchest advocates for all vaccines on the childhood schedule, such as the director of the Center for Infectious Disease Research & Policy, Michael Osterholm, Ph.D., saying that the vote shows federal health authorities can no longer be trusted.
Osterholm, a member of the COVID-19 Advisory Board under the Biden administration, is one of the key players in the “Vaccine Integrity Project,” funded by iAlumbra, a nonprofit founded by Walmart heiress and philanthropist Christy Walton. The project plans to make its own vaccine recommendations.
This Substack is reader-supported.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Vaccine recommendations ‘should not be treated as mandates’
During the day-and-a-half-long discussion about the Hep B vaccine, several committee members, including Dr. Evelyn Griffin, raised concerns that the birth recommendation posed challenges for informed consent, because mothers who had just delivered babies were not in a position to calmly evaluate risks and benefits.
Others, including Levi, argued that the vaccine requirements for children to attend school effectively functioned as mandates.
Liaison members universally disagreed that the recommendations were mandates and argued that ACIP recommendations were really only recommendations, and parents could do what they wanted.
CDC ex officio member, Dr. Adam Langer, who was opposed to changing the recommendation, said that the recommendations had come to function as mandates, but that was not the intention. He proposed the committee make a formal statement that “all vaccine recommendations are recommendations. They should not be treated as mandates.”
He added that mandates put in place by state and local jurisdictions were “problematic.”
“We have a lot of challenges with our culture and our traditions in this country, with telling people what they must and must not do. But that’s not what we’re saying here. We’re saying that at the population level, in the majority of cases, this is what the sign shows is the best practice.”
He said providers should always make the best decision for the individual patient they are working with. “That’s the reason why you’ve been entrusted with a license to practice medicine.”
Watch the ACIP meeting here:
 |

Media bound to pay the price for selling their freedom to (selectively) offend

Sometimes An Ingrate Nation Pt. 2: The Great One Makes His Choice

Recent price declines don’t solve Toronto’s housing affordability crisis

From Exception to Routine. Why Canada’s State-Assisted Suicide Regime Demands a Human-Rights Review
-
 Business2 days ago
Business2 days agoCarney government should privatize airports—then open airline industry to competition
-
 Bruce Dowbiggin16 hours ago
Bruce Dowbiggin16 hours agoIntegration Or Indignation: Whose Strategy Worked Best Against Trump?
-
 Energy2 days ago
Energy2 days agoCanada following Europe’s stumble by ignoring energy reality
-
 COVID-1917 hours ago
COVID-1917 hours agoUniversity of Colorado will pay $10 million to staff, students for trying to force them to take COVID shots
-
 Banks2 days ago
Banks2 days agoTo increase competition in Canadian banking, mandate and mindset of bank regulators must change
-
 Business2 days ago
Business2 days agoLoblaws Owes Canadians Up to $500 Million in “Secret” Bread Cash
-
 Focal Points1 day ago
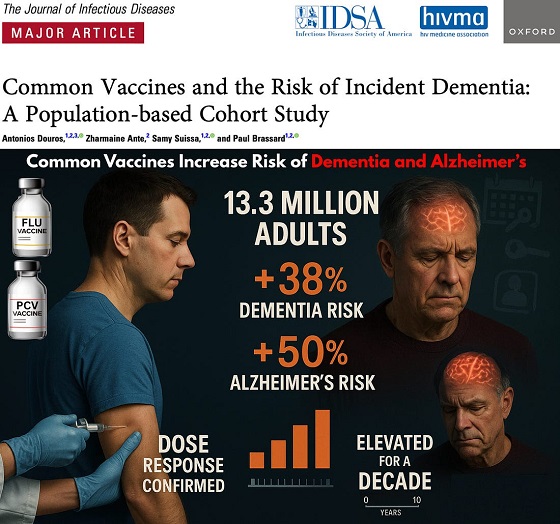
Focal Points1 day agoCommon Vaccines Linked to 38-50% Increased Risk of Dementia and Alzheimer’s
-
 espionage1 day ago
espionage1 day agoWestern Campuses Help Build China’s Digital Dragnet With U.S. Tax Funds, Study Warns