Brownstone Institute
Sweden Did Exceptionally Well During the COVID-19 Pandemic

From the Brownstone Institute
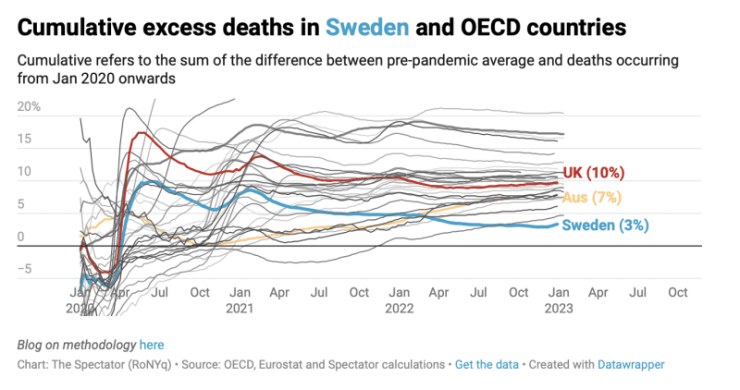
No wonder the news media are totally silent about the data that show that Sweden’s open society policy was what the rest of the world should have done, too. Numerous studies have shown Sweden’s excess death rate to be among the lowest in Europe during the pandemic and in several analyses, Sweden was at the bottom.
This is remarkable considering that Sweden has admitted that it did too little to protect people living in nursing homes.
Unlike the rest of the world, Sweden largely avoided implementing mandatory lockdowns, instead relying on voluntary curbs on social gatherings, and keeping most schools, restaurants, bars and businesses open. Face masks were not mandated and it was very rare to see any Swede dressed as a bank robber.
The Swedish Public Health Agency “gave more advice than threatened punishment” while the rest of the world installed fear in people. “We forbade families to visit their grandmother in the nursing home, we denied men attendance at their children’s births, we limited the number who were allowed to attend church at funerals. Maybe people are willing to accept very strong restrictions if the fear is great enough.”
If we turn to other issues than mortality, it is clear that the harms done by the draconian lockdowns in the rest of the world have been immense in all sorts of ways.
For any intervention in healthcare, we require proof that the benefits exceed the harms. This principle was one of the first and most important victims of the pandemic. Politicians all over the world panicked and lost their heads, and the randomised trials we so badly needed to guide us were never carried out.
We should abbreviate the great pandemic to the great panic.
In my book, “The Chinese virus: Killed millions and scientific freedom,” from March 2022, I have a section about lockdowns.
Lockdown, a questionable intervention
The reborn intolerance toward alternative ideas has been particularly acrimonious in the debate about lockdowns.
There are two main ways to respond to viral pandemics, described in two publications that both came out in October 2020.
The Great Barrington Declaration is only 514 words, with no references. It emphasizes the devastating effects of lockdowns on short- and long-term public health, with the underprivileged disproportionately harmed. Arguing that for children, COVID-19 is less dangerous than influenza, it suggests that those at minimal risk of death should live their lives normally to build up immunity to the virus through natural infection and to establish herd immunity in the society.
It recommends focused protection of the vulnerable. Nursing homes should use staff with acquired immunity and perform frequent PCR testing for COVID-19 of other staff and all visitors. Retired people living at home should have groceries and other essentials delivered to their home and should meet family members outside when possible.
Staying home when sick should be practiced by everyone. Schools, universities, sports facilities, restaurants, cultural activities, and other businesses should be open. Young low-risk adults should work normally, rather than from home.
I have not found anything in the Declaration to be factually wrong.
The other publication is the John Snow Memorandum, which came out two weeks later. Its 945 words are seriously manipulative. There are factual inaccuracies, and several of its 8 references are to highly unreliable science. The authors claim that SARS-CoV-2 has high infectivity, and that the infection fatality rate of COVID-19 is several times higher than that of seasonal influenza.
This is not correct (see Chapter 5), and the two references the authors use are to studies using modelling, which are highly bias-prone.
They also claim that transmission of the virus can be mitigated through the use of face masks, with no reference, even though this was, and still is, a highly doubtful claim.
“The proportion of vulnerable people constitute as much as 30% of the population in some regions.” This was cherry-picking from yet another modelling study whose authors defined increased risk of severe disease as one of the conditions listed in some guidelines. With such a broad definition, it is easy to scare people. However, they did not tell their readers that the modelling study also estimated that only 4% of the global population would require hospital admission if infected,36 which is similar to influenza.
The two declarations did not elicit enlightened debates, but strongly emotional exchanges of views on social media devoid of facts. The vitriolic attacks were almost exclusively directed against those supporting the Great Barrington Declaration, and many people, including its authors, experienced censorship from Facebook, YouTube and Twitter.
The Great Barrington Declaration has three authors; the John Snow Memorandum has 31. The former was published on a website, which is kept alive, the latter in Lancet, which gives its many authors prestige.
In 2021, over 900,000 people had signed the Great Barrington Declaration, including me, as I have always found that the drastic lockdowns we have had, with all its devastating consequences for our societies, were neither scientifically nor ethically justified. I did Google searches to get an idea how much attention the two declarations have had. For the Great Barrington Declaration, there were 147,000 results; for the John Snow Memorandum only 5,500.
The Great Barrington Declaration has not had much political impact. It is much easier for politicians to be restrictive than keeping the societies open. Once a country has taken drastic measures, such as lockdowns and border closings, other countries are accused of being irresponsible if they don’t do the same – even though their effect is unproven. Politicians will not get in trouble for measures that are too draconian, only if it can be argued that they did too little.
In March 2021, Martin Kulldorff and Jay Bhattacharya, two of the three authors of the Great Barrington Declaration, drew attention to some of the consequences of the current climate of intolerance. In many cases, eminent scientific voices have been effectively silenced, often with gutter tactics. People who oppose lockdowns have been accused of having blood on their hands and their university positions threatened.
Many have chosen to stay quiet rather than face the mob, for example Jonas Ludvigsson, after he had published a ground-breaking Swedish study making it clear that it is safe to keep schools open during the pandemic, for children and teachers alike. This was taboo.
Kulldorff and Bhattacharya argued that with so many COVID-19 deaths, most of which have been in old people, it should be obvious that lockdown strategies have failed to protect the old.
The attacks on the Great Barrington Declaration appear to have been orchestrated from the top. On 8 October 2020, Francis Collins, the director of the US National Institutes of Health (NIH), sent a denigrating email to Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases and advisor for several US Presidents, where he wrote:
“This proposal from the three fringe epidemiologists who met with the Secretary seems to be getting a lot of attention – and even a co-signature from Nobel Prize winner Mike Leavitt at Stanford. There needs to be a quick and devastating published take down of its premises. I don’t see anything like that online yet – is it underway?”
Stefan Baral, an epidemiologist from Johns Hopkins, reported that a letter he wrote about the potential harms of population-wide lockdowns in April 2020 was rejected by more than 10 scientific journals and 6 newspapers, sometimes with the pretence that there was nothing useful in it. It was the first time in his career that he could not get a piece placed anywhere.
In September 2021, BMJ allowed Gavin Yamey and David Gorski to publish an attack on the Great Barrington Declaration called, Covid-19 and the new merchants of doubt. A commentator hit the nail when he wrote:
“This is a shoddy smear that is not for publication. The authors have not shown where their targets are scientifically incorrect, they just attack them for receiving funding from sources they dislike or having their videos and comments removed by social media corporations as if that was some indication of guilt.”
Kulldorff has explained what is wrong with the article. They claimed the Declaration provides support to the anti-vaccine movement and that its authors are peddling a “well-funded sophisticated science denialist campaign based on ideological and corporate interests.” But nobody paid the authors any money for their work or for advocating focused protection, and they would not have undertaken it for a professional gain, as it is far easier to stay silent than put your head above the parapet.
Gorski is behaving like a terrorist on social media, and he is perhaps a troll. Without having any idea what I had decided to talk about, or what my motives and background were, he tweeted about me in 2019 that I had “gone full on antivax.” My talk was about why I am against mandatory vaccination for an organisation called Physicians for Informed Consent. Who could be against informed consent? But when I found out who the other speakers were, I cancelled my talk.
In January 2022, Cochrane published a so-called rapid review of the safety of reopening schools or keeping them open. The 38 included studies comprised 33 modelling studies, three observational studies, one quasi‐experimental and one experimental study with modelling components. Clearly, nothing reliable can come out of this, which the authors admitted: “There were very little data on the actual implementation of interventions.”
Using modelling, you can get any result you want, depending on the assumptions you put into the model. But the authors’ conclusion was plain nonsense: “Our review suggests that a broad range of measures implemented in the school setting can have positive impacts on the transmission of SARS‐CoV‐2, and on healthcare utilisation outcomes related to COVID‐19.”
They should have said that since there were no randomised trials, we don’t know if school closures do more good than harm. What they did is what Tom Jefferson has called “garbage in and garbage out … with a nice little Cochrane logo on it.”
About the failing scientific integrity of Cochrane reviews, the funder of the UK Cochrane groups noted in April 2021 that, “This is a point raised by people in the Collaboration to ensure that garbage does not go into the reviews; otherwise, your reviews will be garbage.”
Even though there was nothing to conclude from it, the authors filled 174 pages – about the length of the book you are currently reading – about the garbage they included in their review, which was funded by the Ministry of Education and Research in Germany.
A 2020 rapid systematic review in a medical journal found that school closures did not contribute to the control of the SARS epidemic in China, Hong Kong, and Singapore.
Lockdowns could even make matters worse. If children are sent home to be looked after by their grandparents because their parents are at work, it could bode disaster for the grandparents. Before the COVID-19 vaccines became available, the median age of those who died was 83.
The whole world missed a fantastic opportunity to find out what the truth was by randomising some schools to be closed while keeping others open, but such trials were never done. Atle Fretheim, research director at the Norwegian Institute of Public Health, tried to do a trial but failed. In March 2020, Norwegian government officials were unwilling to keep schools open. Two months later, as the virus waned, they refused to keep schools closed. Norwegian TV shot the messenger: “Crazy researcher wants to experiment with children.” What was crazy was not to do the study. Craziness was also the norm in USA. In many large American cities, bars were open while schools were closed.
When people argue for or against lockdowns and how long they should last and for whom, they are on uncertain ground. Sweden tried to go on with life as usual, without major lockdowns. Furthermore, Sweden has not mandated the use of face masks and very few people have used them.
Author


From the Brownstone Institute
If you want to argue that a mysterious factor X is responsible for the drop in fertility, you will have to explain (1) why the factor affected only the vaccinated, and (2) why it started affecting them at about the time of vaccination.
In January 2022, the number of children born in the Czech Republic suddenly decreased by about 10%. By the end of 2022, it had become clear that this was a signal: All the monthly numbers of newborns were mysteriously low.
In April 2023, I wrote a piece for a Czech investigative platform InFakta and suggested that this unexpected phenomenon might be connected to the aggressive vaccination campaign that had started approximately 9 months before the drop in natality. Denik N – a Czech equivalent of the New York Times – immediately came forward with a “devastating takedown” of my article, labeled me a liar and claimed that the pattern can be explained by demographics: There were fewer women in the population and they were getting older.
To compare fertility across countries (and time), the so-called Total Fertility Rate (TFR) is used. Roughly speaking, it is the average number of children that are born to a woman over her lifetime. TFR is independent of the number of women and of their age structure. Figure 1 below shows the evolution of TFR in several European countries between 2001 and 2023. I selected countries that experienced a similar drop in TFR in 2022 as the Czech Republic.

So, by the end of 2023, the following two points were clear:
- The drop in natality in the Czech Republic in 2022 could not be explained by demographic factors. Total fertility rate – which is independent of the number of women and their age structure – dropped sharply in 2022 and has been decreasing ever since. The data for 2024 show that the Czech TFR has decreased further to 1.37.
- Many other European countries experienced the same dramatic and unexpected decrease in fertility that started at the beginning of 2022. I have selected some of them for Figure 1 but there are more: The Netherlands, Norway, Slovakia, Slovenia, and Sweden. On the other hand, there are some countries that do not show a sudden drop in TFR, but rather a steady decline over a longer period (e.g. Belgium, France, UK, Greece, or Italy). Notable exceptions are Bulgaria, Spain, and Portugal where fertility has increased (albeit from very low numbers). The Human Fertility Project database has all the numbers.
This data pattern is so amazing and unexpected that even the mainstream media in Europe cannot avoid the problem completely. From time to time, talking heads with many academic titles appear and push one of the politically correct narratives: It’s Putin! (Spoiler alert: The war started in February 2022; however, children not born in 2022 were not conceived in 2021). It’s the inflation caused by Putin! (Sorry, that was even later). It’s the demographics! (Nope, see above, TFR is independent of the demographics).
Thus, the “v” word keeps creeping back into people’s minds and the Web’s Wild West is ripe with speculation. We decided not to speculate but to wrestle some more data from the Czech government. For many months, we were trying to acquire the number of newborns in each month, broken down by age and vaccination status of the mother. The post-socialist health-care system of our country is a double-edged sword: On one hand, the state collects much more data about citizens than an American would believe. On the other hand, we have an equivalent of the FOIA, and we are not afraid to use it. After many months of fruitless correspondence with the authorities, we turned to Jitka Chalankova – a Czech Ron Johnson in skirts – who finally managed to obtain an invaluable data sheet.
To my knowledge, the datasheet (now publicly available with an English translation here) is the only officially released dataset containing a breakdown of newborns by the Covid-19 vaccination status of the mother. We requested much more detailed data, but this is all we got. The data contains the number of births per month between January 2021 and December 2023 given by women (aged 18-39) who were vaccinated, i.e., had received at least one Covid vaccine dose by the date of delivery, and by women who were unvaccinated, i.e., had not received any dose of any Covid vaccine by the date of delivery.
Furthermore, the numbers of births per month by women vaccinated by one or more doses during pregnancy were provided. This enabled us to estimate the number of women who were vaccinated before conception. Then, we used open data on the Czech population structure by age, and open data on Covid vaccination by day, sex, and age.
Combining these three datasets, we were able to estimate the rates of successful conceptions (i.e., conceptions that led to births nine months later) by preconception vaccination status of the mother. Those interested in the technical details of the procedure may read Methods in the newly released paper. It is worth mentioning that the paper had been rejected without review in six high-ranking scientific journals. In Figure 2, we reprint the main finding of our analysis.

Figure 2 reveals several interesting patterns that I list here in order of importance:
- Vaccinated women conceived about a third fewer children than would be expected from their share of the population. Unvaccinated women conceived at about the same rate as all women before the pandemic. Thus, a strong association between Covid vaccination status and successful conceptions has been established.
- In the second half of 2021, there was a peak in the rate of conceptions of the unvaccinated (and a corresponding trough in the vaccinated). This points to rather intelligent behavior of Czech women, who – contrary to the official advice – probably avoided vaccination if they wanted to get pregnant. This concentrated the pregnancies in the unvaccinated group and produced the peak.
- In the first half of 2021, there was significant uncertainty in the estimates of the conception rates. The lower estimate of the conception rate in the vaccinated was produced by assuming that all women vaccinated (by at least one dose) during pregnancy were unvaccinated before conception. This was almost certainly true in the first half of 2021 because the vaccines were not available prior to 2021. The upper estimate was produced by assuming that all women vaccinated (by at least one dose) during pregnancy also received at least one dose before conception. This was probably closer to the truth in the second part of 2021. Thus, we think that the true conception rates for the vaccinated start close to the lower bound in early 2021 and end close to the upper bound in early 2022. Once again, we would like to be much more precise, but we have to work with what we have got.
Now that the association between Covid-19 vaccination and lower rates of conception has been established, the one important question looms: Is this association causal? In other words, did the Covid-19 vaccines really prevent women from getting pregnant?
The guardians of the official narrative brush off our findings and say that the difference is easily explained by confounding: The vaccinated tend to be older, more educated, city-dwelling, more climate change aware…you name it. That all may well be true, but in early 2022, the TFR of the whole population dropped sharply and has been decreasing ever since.
So, something must have happened in the spring of 2021. Had the population of women just spontaneously separated into two groups – rednecks who wanted kids and didn’t want the jab, and city slickers who didn’t want kids and wanted the jab – the fertility rate of the unvaccinated would indeed be much higher than that of the vaccinated. In that respect, such a selection bias could explain the observed pattern. However, had this been true, the total TFR of the whole population would have remained constant.
But this is not what happened. For some reason, the TFR of the whole population jumped down in January 2022 and has been decreasing ever since. And we have just shown that, for some reason, this decrease in fertility affected only the vaccinated. So, if you want to argue that a mysterious factor X is responsible for the drop in fertility, you will have to explain (1) why the factor affected only the vaccinated, and (2) why it started affecting them at about the time of vaccination. That is a tall order. Mr. Occam and I both think that X = the vaccine is the simplest explanation.
What really puzzles me is the continuation of the trend. If the vaccines really prevented conception, shouldn’t the effect have been transient? It’s been more than three years since the mass vaccination event, but fertility rates still keep falling. If this trend continues for another five years, we may as well stop arguing about pensions, defense spending, healthcare reform, and education – because we are done.
We are in the middle of what may be the biggest fertility crisis in the history of mankind. The reason for the collapse in fertility is not known. The governments of many European countries have the data that would unlock the mystery. Yet, it seems that no one wants to know.
Author


From the Brownstone Institute
The US Food and Drug Administration (FDA) has approved hundreds of drugs without proof that they work—and in some cases, despite evidence that they cause harm.
That’s the finding of a blistering two-year investigation by medical journalists Jeanne Lenzer and Shannon Brownlee, published by The Lever.
Reviewing more than 400 drug approvals between 2013 and 2022, the authors found the agency repeatedly ignored its own scientific standards.
One expert put it bluntly—the FDA’s threshold for evidence “can’t go any lower because it’s already in the dirt.”
A System Built on Weak Evidence
The findings were damning—73% of drugs approved by the FDA during the study period failed to meet all four basic criteria for demonstrating “substantial evidence” of effectiveness.
Those four criteria—presence of a control group, replication in two well-conducted trials, blinding of participants and investigators, and the use of clinical endpoints like symptom relief or extended survival—are supposed to be the bedrock of drug evaluation.
Yet only 28% of drugs met all four criteria—40 drugs met none.
These aren’t obscure technicalities—they are the most basic safeguards to protect patients from ineffective or dangerous treatments.
But under political and industry pressure, the FDA has increasingly abandoned them in favour of speed and so-called “regulatory flexibility.”
Since the early 1990s, the agency has relied heavily on expedited pathways that fast-track drugs to market.
In theory, this balances urgency with scientific rigour. In practice, it has flipped the process. Companies can now get drugs approved before proving that they work, with the promise of follow-up trials later.
But, as Lenzer and Brownlee revealed, “Nearly half of the required follow-up studies are never completed—and those that are often fail to show the drugs work, even while they remain on the market.”
“This represents a seismic shift in FDA regulation that has been quietly accomplished with virtually no awareness by doctors or the public,” they added.
More than half the approvals examined relied on preliminary data—not solid evidence that patients lived longer, felt better, or functioned more effectively.
And even when follow-up studies are conducted, many rely on the same flawed surrogate measures rather than hard clinical outcomes.
The result: a regulatory system where the FDA no longer acts as a gatekeeper—but as a passive observer.
Cancer Drugs: High Stakes, Low Standards
Nowhere is this failure more visible than in oncology.
Only 3 out of 123 cancer drugs approved between 2013 and 2022 met all four of the FDA’s basic scientific standards.
Most—81%—were approved based on surrogate endpoints like tumour shrinkage, without any evidence that they improved survival or quality of life.
Take Copiktra, for example—a drug approved in 2018 for blood cancers. The FDA gave it the green light based on improved “progression-free survival,” a measure of how long a tumour stays stable.
But a review of post-marketing data showed that patients taking Copiktra died 11 months earlier than those on a comparator drug.
It took six years after those studies showed the drug reduced patients’ survival for the FDA to warn the public that Copiktra should not be used as a first- or second-line treatment for certain types of leukaemia and lymphoma, citing “an increased risk of treatment-related mortality.”
Elmiron: Ineffective, Dangerous—And Still on the Market
Another striking case is Elmiron, approved in 1996 for interstitial cystitis—a painful bladder condition.
The FDA authorized it based on “close to zero data,” on the condition that the company conduct a follow-up study to determine whether it actually worked.
That study wasn’t completed for 18 years—and when it was, it showed Elmiron was no better than placebo.
In the meantime, hundreds of patients suffered vision loss or blindness. Others were hospitalized with colitis. Some died.
Yet Elmiron is still on the market today. Doctors continue to prescribe it.
“Hundreds of thousands of patients have been exposed to the drug, and the American Urological Association lists it as the only FDA-approved medication for interstitial cystitis,” Lenzer and Brownlee reported.
“Dangling Approvals” and Regulatory Paralysis
The FDA even has a term—”dangling approvals”—for drugs that remain on the market despite failed or missing follow-up trials.
One notorious case is Avastin, approved in 2008 for metastatic breast cancer.
It was fast-tracked, again, based on ‘progression-free survival.’ But after five clinical trials showed no improvement in overall survival—and raised serious safety concerns—the FDA moved to revoke its approval for metastatic breast cancer.
The backlash was intense.
Drug companies and patient advocacy groups launched a campaign to keep Avastin on the market. FDA staff received violent threats. Police were posted outside the agency’s building.
The fallout was so severe that for more than two decades afterwards, the FDA did not initiate another involuntary drug withdrawal in the face of industry opposition.
Billions Wasted, Thousands Harmed
Between 2018 and 2021, US taxpayers—through Medicare and Medicaid—paid $18 billion for drugs approved under the condition that follow-up studies would be conducted. Many never were.
The cost in lives is even higher.
A 2015 study found that 86% of cancer drugs approved between 2008 and 2012 based on surrogate outcomes showed no evidence that they helped patients live longer.
An estimated 128,000 Americans die each year from the effects of properly prescribed medications—excluding opioid overdoses. That’s more than all deaths from illegal drugs combined.
A 2024 analysis by Danish physician Peter Gøtzsche found that adverse effects from prescription medicines now rank among the top three causes of death globally.
Doctors Misled by the Drug Labels
Despite the scale of the problem, most patients—and most doctors—have no idea.
A 2016 survey published in JAMA asked practising physicians a simple question—what does FDA approval actually mean?
Only 6% got it right.
The rest assumed that it meant the drug had shown clear, clinically meaningful benefits—such as helping patients live longer or feel better—and that the data was statistically sound.
But the FDA requires none of that.
Drugs can be approved based on a single small study, a surrogate endpoint, or marginal statistical findings. Labels are often based on limited data, yet many doctors take them at face value.
Harvard researcher Aaron Kesselheim, who led the survey, said the results were “disappointing, but not entirely surprising,” noting that few doctors are taught about how the FDA’s regulatory process actually works.
Instead, physicians often rely on labels, marketing, or assumptions—believing that if the FDA has authorized a drug, it must be both safe and effective.
But as The Lever investigation shows, that is not a safe assumption.
And without that knowledge, even well-meaning physicians may prescribe drugs that do little good—and cause real harm.
Who Is the FDA Working for?
In interviews with more than 100 experts, patients, and former regulators, Lenzer and Brownlee found widespread concern that the FDA has lost its way.
Many pointed to the agency’s dependence on industry money. A BMJ investigation in 2022 found that user fees now fund two-thirds of the FDA’s drug review budget—raising serious questions about independence.

Yale physician and regulatory expert Reshma Ramachandran said the system is in urgent need of reform.
“We need an agency that’s independent from the industry it regulates and that uses high-quality science to assess the safety and efficacy of new drugs,” she told The Lever. “Without that, we might as well go back to the days of snake oil and patent medicines.”
For now, patients remain unwitting participants in a vast, unspoken experiment—taking drugs that may never have been properly tested, trusting a regulator that too often fails to protect them.
And as Lenzer and Brownlee conclude, that trust is increasingly misplaced.
- Investigative report by Jeanne Lenzer and Shannon Brownlee at The Lever [link]
- Searchable public drug approval database [link]
- See my talk: Failure of Drug Regulation: Declining standards and institutional corruption
Republished from the author’s Substack
Author



Before Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually

FDA requires new warning on mRNA COVID shots due to heart damage in young men

Canada’s euthanasia regime is already killing the disabled. It’s about to get worse

Blackouts Coming If America Continues With Biden-Era Green Frenzy, Trump Admin Warns
-
Fraser Institute2 days ago
Before Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually
-
MAiD2 days ago
Canada’s euthanasia regime is already killing the disabled. It’s about to get worse
-
 Frontier Centre for Public Policy2 days ago
Frontier Centre for Public Policy2 days agoNew Book Warns The Decline In Marriage Comes At A High Cost
-
 Business2 days ago
Business2 days agoPrime minister can make good on campaign promise by reforming Canada Health Act
-
 Addictions1 day ago
Addictions1 day ago‘Over and over until they die’: Drug crisis pushes first responders to the brink
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV
-
 Daily Caller1 day ago
Daily Caller1 day agoUSAID Quietly Sent Thousands Of Viruses To Chinese Military-Linked Biolab
-
 Energy2 days ago
Energy2 days agoLNG Export Marks Beginning Of Canadian Energy Independence