COVID-19
Neil Macdonald asks the most important COVID-19 question of all

This is posted with permission from the author, Neil MacDonald. It is originally posted at neilmacdonald.me
So. Who gets the ventilators?
I wish Sophie Gregoire Trudeau good health, and a complete recovery in her quarantine. The same for the lovely Margaret Trudeau, if she comes down with COVID-19. Both women were at the same speaking engagement in London; presumably, that is where Madame Gregoire Trudeau contracted the virus.
If, heaven forfend, either woman develops the sort of severe respiratory difficulties that have killed other COVID-19 patients, I hope they will both have access to peerless medical care, and a ventilator. Actually, I am certain they will.
One is the prime minister’s wife, the other his mother. Privilege has its privileges.
At the same time – and here comes the kicker – I am not at all certain that, if I or any of my aged relatives come down with the disease in the uncertain and increasingly terrifying weeks to come, there will be ventilators for us. And as one American epidemiologist put it recently, the alternative to ventilation for someone with extreme respiratory symptoms is death. As a despairing Italian physician put it on social media from the horrors of his triage centre in Bergamo: “Every ventilator becomes like gold.”
Here is the math: Health Minister Patty Hajdu says between 30 and 70 per cent of Canadians will likely be infected. The mortality rate of COVID-19 is between two and three per cent. Assuming the optimistic end of Hajdu’s estimate, and the optimistic end of the mortality rate, we are still talking about 225,000 people dying, and, as the despairing Italian physician says, the diagnosis is always the same: Bilateral interstitial pneumonia. Meaning those patients’ lungs are so badly compromised the only thing that has a chance of saving them is a ventilator, or mechanical breathing apparatus. It alone can infuse the lungs with enough oxygen to maintain life.
Now: We are told Canada has about 5,000 ventilators. That’s one ventilator for every 45 of those dying patients. Unless Canada somehow acquires a lot more of the machines, and the entire world is now chasing them, there will be rationing. That is what has been happening in Italy. Doctors there have been given the ghastly job of deciding who receives ventilation, and who is sent home to meet their fate.
Now, let’s add something else to the equation: In Canada, the law prevents citizens from paying for core medical care, which a ventilator surely is. In principle, ventilators will be rationed, well, rationally.
But that’s not how the system really works.
In Canada, influence and power get you to the front of the line. Does anyone really believe that cabinet ministers or premiers or captains of industry or very senior government officials sit in waiting rooms, or have a hard time finding a family doctor? Or that those of us with professional or family connections aren’t treated as privileged entities?
So the big question – the crucial, life-or-death question as this virus tears through the population – will very quickly be this: who gets the ventilators?
No doubt, an attempt will be made to lay down a set of objective criteria. They probably already exist. It makes sense to ventilate patients who stand the best chance of surviving. A physician friend in Italy unilaterally decided to send very old people home, along with anyone whose health was already severely compromised by previous morbidities.
But imagine the pressure on a Canadian doctor, or hospital dependent on government funding, when the aged relative of a very powerful politician needs ventilation. Or a very rich person who has donated generously to the hospital. Or the mother or father of a person whose role in the economy is considered so crucial that he or she must not be distracted by familial worries.
Jane Philpott, Justin Trudeau’s first health minister, once declared that not being able to buy your way to the front of the line is a “core Canadian value.” The remark was rather gormless, I thought at the time, given the reality of the system. Doctor friends of mine thought it was hysterical.
But the big test is coming. The public deserves to know precisely how lifesaving care will be allocated. The public has a right to transparent fairness.
My guess: fairness and objective allocation of resources will slam into the wall of privilege. We shall see. We shall also see how intrepid the media is on this subject. So far, it hasn’t been.
From neilmacdonald.me

Neil Macdonald spent 43 years reporting on politics, wars, elections, revolutions, booms, crashes, coups, and the struggles of ordinary human beings in the unforgiving, bewildering rush of history.
He worked as an editor and reporter in three newspapers before moving to CBC News, for which he covered Quebec before moving to Parliament Hill, then abroad as a foreign correspondent in the Middle East and Washington, DC., and finally as the CBC’s opinion columnist.
He has stood in Iraq watching missiles strike, in Bethlehem watching people welcome the new millennium, in Jerusalem watching an intifada erupt, and in Chicago watching Barack Obama accept the American presidency. He followed the Pope through the Holy Land, tracked down Hitler’s last general in Europe, covered the triumphant arrival and subsequent humiliation of Jean-Bertrand Aristide in Haiti, revealed the plotters who killed Rafiq Hariri in Beirut, and documented the financial horrors unleashed on America’s cities by Wall Street.
He speaks French, having grown up in Quebec, reasonably good English, and sufficient Arabic. He lives in Ottawa.
Learning at home? Here’s a list of links to take you on a “Virtual Field Trip”

 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
As millions of Americans anxiously await action from the new HHS leadership against the COVID-19 mRNA injections—injected into over 9 million children this year—Robert F. Kennedy Jr. has finally gone publicly on the offensive:
Let’s go over each key point made by RFK Jr.:
The recommendation for children was always dubious. It was dubious because kids had almost no risk for COVID-19. Certain kids that had very profound morbidities may have a slight risk. Most kids don’t.
In the largest review to date on myocarditis following SARS-CoV-2 infection vs. COVID-19 vaccination, Mead et al found that vaccine-induced myocarditis is not only significantly more common but also more severe—particularly in children and young males. Our findings make clear that the risks of the shots overwhelmingly outweigh any theoretical benefit:
 |
The OpenSAFELY study included more than 1 million adolescents and children and found that myocarditis was documented ONLY in COVID-19 vaccinated groups and NOT after COVID-19 infection. There were NO COVID-19-related deaths in any group. A&E attendance and unplanned hospitalization were higher after first vaccination compared to unvaccinated groups:
So why are we giving this to tens of millions of kids when the vaccine itself does have profound risk? We’ve seen huge associations of myocarditis and pericarditis with strokes, with other injuries, with neurological injuries.
The two largest COVID-19 vaccine safety studies ever conducted, involving 99 million (Faksova et al) and 85 million people (Raheleh et al), confirm RFK Jr.’s concerns, documenting significantly increased risks of serious adverse events following vaccination, including:
- Myocarditis (+510% after second dose)
- Acute Disseminated Encephalomyelitis (+278% after first dose)
- Cerebral Venous Sinus Thrombosis (+223% after first dose)
- Guillain-Barré Syndrome (+149% after first dose)
- Heart Attack (+286% after second dose)
- Stroke (+240% after first dose)
- Coronary Artery Disease (+244% after second dose)
- Cardiac Arrhythmia (+199% after first dose)
 |
And this was clear even in the clinical data that came out of Pfizer. There were actually more deaths. There were about 23% more deaths in the vaccine group than the placebo group. We need to ask questions and we need to consult with parents.
Actually, according to the Pfizer’s clinical trial data, there were 43% more deaths in the vaccine group compared to the placebo group when post-unblinding deaths are included:
 |
We need to give people informed consent, and we shouldn’t be making recommendations that are not good for the population.
Public acknowledgment of the grave harms of COVID-19 vaccines signals that real action is right around the corner. However, we must hope that action is taken for ALL age groups, as no one is spared from their life-reducing effects:
Alessandria et al (n=290,727, age > 10 years): People vaccinated with 2 doses lost 37% of life expectancy compared to the unvaccinated population during follow-up.
 |
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.


 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
45.3% of “COVID-19 deaths” in Greece had no symptoms — exposing the coordinated PSYOP deployed to maximize fear and enforce mass compliance with draconian control measures.
The study titled “Deaths “due to” COVID-19 and deaths “with” COVID-19 during the Omicron variant surge, among hospitalized patients in seven tertiary-care hospitals, Athens, Greece” was just published in the journal Scientific Reports:
Abstract
In Greek hospitals, all deaths with a positive SARS-CoV-2 test are counted as COVID-19 deaths. Our aim was to investigate whether COVID-19 was the primary cause of death, a contributing cause of death or not-related to death amongst patients who died in hospitals during the Omicron surge and were registered as COVID-19 deaths. Additionally, we aimed to analyze the factors associated with the classification of these deaths. We retrospectively re-viewed all in-hospital deaths, that were reported as COVID-19 deaths, in 7 hospitals, serving Athens, Greece, from January 1, 2022, until August 31, 2022. We retrieved clinical and laboratory data from patient records. Each death reported as COVID-19 death was characterized as: (A) death “due to” COVID-19, or (B) death “with” COVID-19. We reviewed 530 in-hospital deaths, classified as COVID-19 deaths (52.4% males; mean age 81.7 ± 11.1 years). We categorized 290 (54.7%) deaths as attributable or related to COVID-19 and in 240 (45.3%) deaths unrelated to COVID-19. In multivariable analysis The two groups differed significantly in age (83.6 ± 9.8 vs. 79.9 ± 11.8, p = 0.016), immunosuppression history (11% vs. 18.8%, p = 0.027), history of liver disease (1.4% vs. 8.4%, p = 0.047) and the presence of COVID-19 symptoms (p < 0.001). Hospital stay was greater in persons dying from non-COVID-19 related causes. Among 530 in-hospital deaths, registered as COVID-19 deaths, in seven hospitals in Athens during the Omicron wave, 240 (45.28%) were reassessed as not directly attributable to COVID-19. Accuracy in defining the cause of death during the COVID-19 pandemic is of paramount importance for surveillance and intervention purposes.
 |
Key Findings:
Massive Overcounting of COVID-19 Deaths
- Out of 530 hospital deaths registered as COVID-19 deaths, only 290 (54.7%) were actually caused by COVID-19.
- 240 deaths (45.3%) were found to be completely unrelated to COVID-19 — patients died with a positive PCR test, but showed no symptoms, required no COVID-specific treatment, and died of clearly unrelated causes.
Death Certificate Inaccuracy
- Of the 204 certificates listing COVID-19 as the direct cause of death, only 132 (64.7%) were confirmed as such after clinical review.
- Of the 324 certificates listing COVID-19 as a contributing factor, only 86 (26.5%) were found to be truly related.
Hospital-Acquired Infections Misclassified
- Patients infected during hospitalization were significantly more likely to be misclassified as COVID-19 deaths (OR: 2.3, p = 0.001).
Younger Age and Severe Comorbidities Associated with Misclassification
- Patients who died “with” COVID-19 were younger, more likely to be immunosuppressed, have end-stage liver disease, or be admitted for other causes.
Symptoms and Treatments Differed Sharply
Patients who died “due to” COVID-19 were more likely to:
- Exhibit classic symptoms: hypoxia (44.1%), shortness of breath, fever, and cough
- Require oxygen support (93.4% vs. 66.9%) and receive COVID-specific therapies:
- Remdesivir (5-day course: 61.9% vs. 35.2%)
- Dexamethasone (81.7% vs. 40.7%)
Study Strengths
This study went far beyond death certificate coding, implementing a rigorous, multi-source clinical audit:
- Full medical chart reviews: Included physician notes, lab data, imaging, and treatment records.
- Attending physician interviews: Structured questionnaires captured real-time clinical insights from those who treated the patients.
- Dual independent expert assessments: Two experienced infectious disease specialists (each with >2,500 COVID cases) reviewed each case independently for classification accuracy.
This study found that nearly half of all registered COVID-19 deaths during the Omicron wave in Greece were misclassified, with no clinical evidence linking them to COVID-19 as the true cause. Given that similar death coding practices were employed across Western nations, it is reasonable to conclude that COVID-19 death counts were artificially inflated to a comparable degree elsewhere.
This drastic inflation of death counts aligns with what many now understand to be a coordinated psychological operation (PSYOP)—designed to instill fear and maximize compliance with draconian pandemic measures such as lockdowns, mask mandates, and mass mRNA injection campaigns.
It is this weaponization of fear that has prompted criminal referrals in seven U.S. states, triggering active criminal investigations into top COVID-19 officials for terrorism, murder and racketeering:
BREAKING – The Pandemic Justice Phase Begins as Criminal Investigations Commence |
||||||
|
||||||
 |
||||||
|
By Nicolas Hulscher, MPH
|
||||||
|
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.



Province to expand services provided by Alberta Sheriffs: New policing option for municipalities

Made in Alberta! Province makes it easier to support local products with Buy Local program
Is HNIC Ready For The Winnipeg Jets To Be Canada’s Heroes?

CSIS Warned Beijing Would Brand Conservatives as Trumpian. Now Carney’s Campaign Is Doing It.
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoOttawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoBREAKING: THE FEDERAL BRIEF THAT SHOULD SINK CARNEY
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoHow Canada’s Mainstream Media Lost the Public Trust
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoReal Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoCHINESE ELECTION THREAT WARNING: Conservative Candidate Joe Tay Paused Public Campaign
-
 Media1 day ago
Media1 day agoCBC retracts false claims about residential schools after accusing Rebel News of ‘misinformation’
-
 John Stossel1 day ago
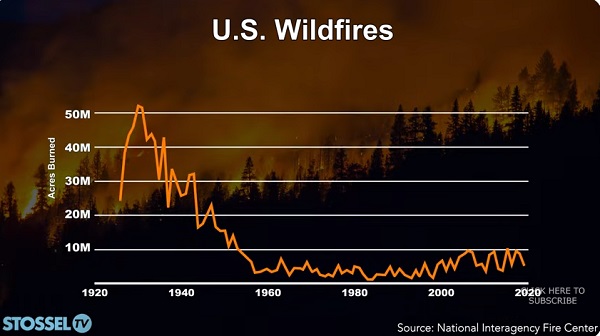
John Stossel1 day agoClimate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
COVID-192 days ago
Nearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal