MAiD
Skiing down euthanasia’s slippery slope

From the Macdonald Laurier Institute
By John Keown
Canada is on track to surpass the Netherlands.
When the Canadian Parliament legalized voluntary euthanasia (VE) and physician-assisted suicide (PAS) in 2016, at the behest of the Supreme Court, supporters of legalization doubtless hoped the new law and its operation would prove something of a poster child for the compassionate and controlled medical ending of life. Its critics, however, might now describe it as less like a poster child and more like the picture of Dorian Gray.
Whether the law should permit VE and PAS is one of the most important questions of social policy in developed countries. Here we will eschew the tendentious and misleading euphemisms “assisted dying” and “medical assistance in dying.” The law and professional medical ethics have always allowed doctors and nurses to “help people to die” by palliating symptoms, even if so doing foreseeably shortens life. What the new law permits is radically different: the intentional killing of patients and intentionally assisting them to kill themselves.
Moreover, the euthanasia law does not require that patients be “dying” or “terminally ill” in order (to employ further euphemisms) to be given the “medication” for such “treatment.” Policy makers should not disguise, or be complicit in disguising, the foundational nature of this moral, legal, medical, and social paradigm shift.
The Canadian experience with VE and PAS is of major relevance to the international debate. Does it support the assurances of legalization campaigners that these practices can be effectively controlled by the law and provide a “last resort” in the sort of “hard cases” involving patients who are (or who fear) dying in severe pain or discomfort – patients who are so regularly paraded before us by the mass media?
Or does it support the counter-argument that the appropriate answer to such pain and discomfort is the wider availability of quality palliative care, and that a relaxed law would not only fail to prevent mistake or abuse but would also prove a first step on a precipitous “slippery slope” to VE and PAS in an ever-widening range of cases?
The best body of evidence concerning the effects of legalization comes from the Netherlands, whose experience I have studied for 35 years.
The Dutch Supreme Court declared VE and PAS lawful in 1984. To justify this change, the Dutch invoked the doctor’s duty to relieve suffering, and the focus of discussion was the physical suffering of the dying. However, in 1994 the same court held that the requirement of “unbearable suffering” could be satisfied by an illness that was neither terminal nor even physical and was solely mental. (Whether the patient’s suffering was “unbearable” remains very largely a subjective matter decided by the patient.)
In 2016 the Dutch government proposed a further legal extension: to elderly folk with a “completed” life. And, if some patients still do not manage to meet the lax legal criteria for VE and PAS their doctors can, and do, advise them that there is the option of being medically palliated while they dehydrate themselves to death.
Lethal injections have even been extended to patients who are incapable of making a request. In 1996 the Dutch courts declared it lawful intentionally to kill disabled infants, such as those with spina bifida. And only last year, the government announced that euthanasia would be allowed for children between one and 12. In short, over the past 40 years the Dutch have clearly tumbled down euthanasia’s slippery slope. Their Belgian neighbours, who followed them in 2002 (the same year that Dutch legislation enshrining the pre-existing legal criteria came into force) are also on the skids.
Why does this happen? There are two explanations, one empirical, the other logical. The empirical explanation is that relaxed laws cannot effectively control VE and PAS in practice because the challenges of formulating, drafting, and enforcing proper safeguards are intractable. Common media references to “strict safeguards” in places like the Netherlands and Canada reflect journalistic ignorance rather than social reality.
The second explanation is logical. VE and PAS are, campaigners tell us, justified by (i) respect for patient autonomy and (ii) by the duty to relieve suffering. But if one buys their argument, euthanasia is also justified for competent patients who are suffering from chronic, not merely terminal, illness, and whether their suffering is physical or mental. Suffering is suffering, whether from terminal cancer or chronic arthritis or depression. Indeed, suffering from chronic illness, physical or mental, may last a lifetime, not merely a few weeks or months. And why exclude the perduring existential suffering that tragically blights the lives of so many lonely, elderly folk?
Why, moreover, exclude euthanasia for suffering patients such as infants who are incapable of requesting death (non-voluntary euthanasia or NVE)? The absence of patient autonomy does not cancel the doctor’s duty of beneficence.
The Dutch have, then, proved nothing if not logical, and it is surely only a matter of time until their law is formally extended to embrace the elderly who are “tired of life.”
And so, to Canada. It leaped onto the slope as a result of the Supreme Court’s ruling in Carter v. Canada in 2015, in which the court overruled its previous decision in Rodriguez v. British Columbia in 1993. Rodriguez was soundly reasoned, and its reasoning remains in line with the rejection of a right to VE and PAS by the highest courts in other common law jurisdictions including the United States, the United Kingdom, and Ireland. By contrast (as I explain in Euthanasia, Ethics and Public Policy), Carter may strike some as reading more like rationalization than reasoning and as an exercise in judicial activism that stains Canadian jurisprudence.
Here we will mention just one of its flaws: its endorsement of the crucial finding of the trial judge that the evidence from jurisdictions with VE and/or PAS showed that the risks of legalization can be very largely avoided by carefully designed, well-monitored safeguards. This finding bristled with problems, not least of which was that no jurisdiction had (or has) carefully designed, well-monitored safeguards.
In a subsequent and similar case in Ireland, three senior judges carefully reviewed the judgment of the trial judge in Carter. They unanimously rejected her finding, not least in view of the (undisputed) evidence from the Netherlands and Belgium of the striking extent of medical euthanasia without any explicit request from the patient.
I was called as an expert witness in Carter by the Attorney General of Canada. At the end of my day-long cross-examination in Vancouver by the late Joseph Arvay, Q.C., counsel for those challenging the law against VE and PAS, the judge asked me to reprise both the practical and logical slippery slope arguments that I have outlined above. I did so, using the evidence from the Netherlands, Belgium, and Oregon to demonstrate the lack of effective legal control, and the Dutch endorsement of infanticide to illustrate the logical slippery slope. (Indeed, the two leading ethics experts called by Mr Arvay had endorsed both voluntary and non-voluntary euthanasia in their published work.)
The judge nevertheless concluded that the evidence showed that VE and PAS could safely be legalized. As for the logical argument, she dismissed it as involving “speculation” and because the legal challenge was only to the legal prohibition as it affected competent patients! Her failure to join the dots was noteworthy. (My 2022 paper in the Cambridge Law Journal confirms the real, not speculative, nature of the logical argument.) The Supreme Court endorsed the judge’s several errors. It did so, moreover, without even the fig leaf of a single dissenting judgment.
And what have we (all too predictably) witnessed since 2016, when legislation accommodated the Supreme Court’s ruling? Even leaving aside the steep yearly increases in the number of medical killings, we have seen that the statutory requirement that the patient’s death be “reasonably foreseeable” need no longer be met; that euthanasia where the sole cause of suffering is mental illness has been approved (though its implementation has been delayed until 2027 to allow preparations to be made), and that further expansion of the law to include “mature” minors, and requests for euthanasia written in advance of incompetence, is on the cards. Not to mention the several reported cases involving vulnerable patients that raise unsettling questions about the operation of the law.
In 1994 a distinguished House of Lords Select Committee on Medical Ethics unanimously concluded that English law should not permit VE or PAS. The committee observed that the criminal law’s prohibition on intentional killing was the “cornerstone of law and of social relationships” that “protects each one of us impartially, embodying the belief that all are equal.”
The experience in Canada uncomfortably confirms what happens once a society abandons that historic, bright-line prohibition in favour of the competing and arbitrary notion that whereas some people have lives that are “worth living,” others would be “better off dead” and it is right to grant their request to be killed or to help them kill themselves.
It is surely only a matter of time until calls are made for the “benefit” of a hastened death to be conferred on people who are incapable of requesting it. Why “discriminate” against people who are suffering with, say, advanced dementia merely because they are incapable of requesting a lethal injection? Why deny them their rights under the Canadian Charter of Rights and Freedoms? The enormous cost savings will lurk supportively behind the argument, like a gangster’s heavy.
In the Netherlands, euthanasia has been normalized to a significant degree. Far from being an exceptional practice in “hard cases” of “last resort,” it has come to be regarded largely as another healthcare option. Canada appears to be following suit. Professor Trudo Lemmens, the eminent Canadian health lawyer, has noted the “troubling normalization” of euthanasia in Canada where, he adds, “rights rhetoric” surrounding the issue has replaced evidence-based debate.
Thankfully, the concerning developments in Canada are now being ventilated in the public domain: in the media, both in Canada and abroad; in journals of law, medicine and bioethics, and by the UN rapporteur on the rights of people with disabilities. It is telling that in the UK even campaigners for legalization are straining to distance themselves from the Canadian precedent.
In 40 years, the Dutch have slid down the slippery slope. In fewer than 10, Canada appears to be veritably skiing.
John Keown DCL (Oxon) is the Rose F. Kennedy Professor of Christian Ethics in the Kennedy Institute of Ethics at Georgetown University in Washington, DC. He previously taught medical law at the University of Cambridge. The second edition of his book Euthanasia, Ethics and Public Policy: An Argument Against Legalisation, described as “magisterial” by Lord Judge, the former Lord Chief Justice of England and Wales, was published by Cambridge University Press in 2018.

From LifeSiteNews
Even the UN has described Canada’s assisted suicide program as ‘state-sponsored eugenics’ and called upon the government to curtail plans to expand euthanasia access.
In Canada, we kill the disabled. Over 90 percent of babies diagnosed with Down syndrome in the womb are aborted; pre-born children diagnosed with other disabilities usually meet the same fate. But for decades, our Nazi-style lethal ableism was limited to those not yet born.
With the expansion of euthanasia eligibility to those suffering solely from disability or mental illness scheduled to come into effect in 2027, that is slated to change. Disability groups have been nearly unanimous in their condemnation of this plan, which has been delayed twice by the Liberal government due to pushback from across Canadian society – but not cancelled entirely.
Even the United Nations Committee on the Rights of Persons with Disabilities, examining Canada’s compliance with the U.N. Conventions on the Rights of Persons with Disabilities earlier this year, concluded that Canada was embarking on “state-sponsored eugenics” and called on the Canadian government to scrap these plans and roll back the expanding euthanasia regime. The disability rights group Inclusion Canada, as well as several others, had written to the body to sound the alarm about Canada’s euthanasia policies.
Canadians with physical disabilities have been attempting to get the government’s attention for years, with stories of those who seeking euthanasia because they cannot get the support or care they need periodically dominating international headlines. (This ugly reality is best encapsulated in a famous cartoon showing stairs leading to a healthcare provider, with the only wheelchair ramp leading to “euthanasia.”) These stories have not yet been heeded by the government.
A story recently posted to X by Samantha Smith, a victim advocate and survivor of the grooming and rape gangs in the U.K., highlights Canada’s grim slippery slope. It is worth reading in full:
A family member of mine is a nurse in Canada. They performed several assisted dying procedures at the care home they worked at, before refusing to continue. In one case, the family of a mentally disabled man decided they wanted him to be euthanised. He didn’t want to die. But my family member was legally forced to end his life. They held his hand while he told them “I’m hungry” and “I’m thirsty.”
That poor man didn’t understand what was happening to him as he was pumped full of medication that would end his life, and my family member wept for the soul that was being lost unnecessarily. He wasn’t terminally ill. He wasn’t particularly old. He wasn’t dying. He didn’t want to die. But he didn’t have a choice. Because his life was deemed dispensable by his family, and the Government gave them the power to end his life regardless of his needs or wishes.
And when my family member told their workplace that they couldn’t continue performing these procedures – that their conscience wouldn’t allow it – they were told that it was their “legal duty” as a nurse. They still refused. But not everyone will have the moral fibre or bravery of my family member.
The road to hell is paved with good intentions, and this is exactly what the Assisted Dying Bill opens the door to. It starts with “choice” and “dignity.” But suicide isn’t only done “when the patient wants it.” And the countries where it is already legalised have shown us the grim reality. In the Netherlands, 40% of euthanasia deaths occur without patient consent. In Canada, it has been offered to Paralympians who only asked for a mobility aid. If it can happen there; it will happen here. People will be killed against their will.
When asked for public corroboration, Smith stated: “No, my family member will not ‘go public.’ Yes, I trust his testimony. No, he is not a horrible, awful person. Yes, this is really happening. The black letter law vs. the grim reality are two very different things. Just because the law was supposed to protect against coercion or non-consenting procedures … doesn’t mean it is.”
I wish I didn’t believe her, but I do. I believe her because euthanasia providers have ended the lives of people like Alan Nichols, who was taken to the hospital by family members after a psychiatric episode and euthanized days later. I believe her because leaked documents show that Ontario’s euthanasia providers have tracked 428 cases of possible criminal violations without a single case being referred to law enforcement. I believe her because Canada’s medical establishment already embraces lethal ableism, and our government does too.
Canada is already killing those with disability or mental illness; thus far, euthanasia practitioners are forced to come up with other reasons for doing so (the written reason for Alan Nichols’ lethal injection was “hearing loss”). But once eligibility requirements are expanded in 2027, the floodgates will open. There is still time to stop this expansion, and we must doing everything we can to do so. The lives of people with disabilities depend on it.


From LifeSiteNews
After ten years of assisted suicide, Canada has become synonymous with grim stories of death by lethal injection, with the regime’s net growing ever wider.
When Justin Trudeau took power in 2015, he announced that Canada was back and that his election was a harbinger of “sunny ways” and a new era for the country.
It was a new era, alright, but the ways turned out not to be sunny. In his ten years in office, over 60,000 Canadians were euthanized under the regime that his government brought in, and overnight, Canada became an international cautionary tale.
International headlines highlighted the grim story of Canada, where people were getting lethal injections because they were disabled; because they couldn’t get cancer treatment; because they were veterans with PTSD. As the U.K.’s Spectator asked in a chilling 2022 headline: “Why is Canada euthanizing the poor?”
READ: New Conservative bill would ban expansion of euthanasia to Canadians suffering mental illness
Indeed, in the United Kingdom – where Labour MP Kim Leadbeater’s dystopian assisted suicide bill passed last week – Canada was seen as so objectively horrifying that euthanasia advocates insisted that comparisons to their Commonwealth neighbor constituted fearmongering. Leadbeater, in fact, stated that her bill is “worlds apart” from Canada’s euthanasia regime. Anyone advocating for euthanasia must now reckon with Canada, which highlights how short and slick the slope really is.
Earlier this month, the New York state legislature also passed a bill legalizing assisted suicide; assisted suicide laws are also being considered in Maryland and Illinois. On June 14, the New York Times published a powerful op-ed by Ross Douthat titled “Why the Euthanasia Slope Is Slippery.” As is now standard in the international press, Canada’s euthanasia regime came up.
“A few days before the vote, my colleague Katie Engelhart published a report on the expansive laws allowing ‘medical assistance in dying’ in Canada,” Douthat wrote, “which were widened in 2021 to allow assisted suicide for people without a terminal illness, detailing how they worked in the specific case of Paula Ritchie, a chronically ill Canadian euthanized at her own request.”
“Many people who support assisted suicide in terminal cases have qualms about the Canadian system,” Douthat continued. “So it’s worth thinking about what makes a terminal-illness-only approach to euthanasia unstable, and why the logic of what New York is doing points in a Canadian direction even if the journey may not be immediate or direct.”
Notice, here, that a columnist can refer to the “Canadian direction” with the assumption that everybody recognizes, without question, that this a particularly bad direction to be heading in. Even euthanasia advocates, while privately admiring the scale and efficiency of the Canadian killing fields, feel it necessary to distance themselves from Canada publicly.
Douthat noted that the Canadian example reveals why the slippery slope is inevitable; that people have essentially come to expect that doctors “always need to offer something,” and that when no further care or treatment is possible, that assisted suicide should be available. This logic “assumes that the dying have entered a unique zone where the normal promises of medicine can no longer be kept, a state of exception where it makes sense to license doctors to deliver death as a cure.” But Douthat observes:
The problem is that a situation where the doctor tells you that there’s nothing more to be done for you is not really exceptional at all. Every day, all kinds of people are told that their suffering has no medical solution: people with crippling injuries, people with congenital conditions and people … with an array of health problems whose etiology science does not even understand.
READ: Cardinal Dolan denounces New York assisted suicide bill as ‘cheapening of human life’
The logic of assisted suicide means that inevitably, eligibility will expand to all kinds of suffering.
“Suffering is general and not limited, the dying are not really a category unto themselves, and the case for a lethal solution will creep beyond the bounds you set,” Douthat concluded. “In the end, you can have a consensus that suicide is intrinsically wrong, that suffering should be endured to whatever end and that doctors shouldn’t kill you. Or you can have an opening to death that will be narrow only at the start – and in the end, a wide gate through which many, many people will be herded.”
How do we know? Well, Douthat writes, “The Canadian experience shows this clearly.” After ten years of sunny ways, “Canada” has become synonymous with grim stories of death by lethal injection.




RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
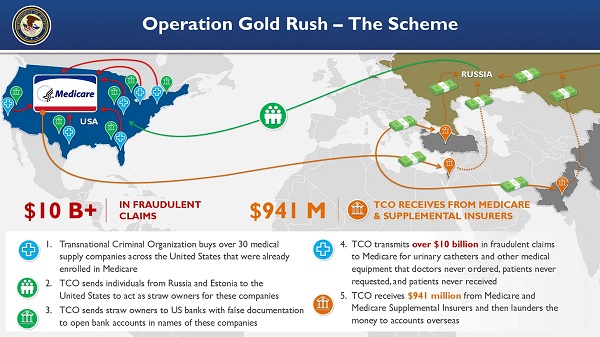
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Crime1 day ago
Crime1 day ago“This is a total fucking disaster”
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV
-
 Fraser Institute1 day ago
Fraser Institute1 day agoBefore Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually
-
 Daily Caller2 days ago
Daily Caller2 days agoBlackouts Coming If America Continues With Biden-Era Green Frenzy, Trump Admin Warns
-
MAiD1 day ago
Canada’s euthanasia regime is already killing the disabled. It’s about to get worse
-
 Daily Caller2 days ago
Daily Caller2 days ago‘I Know How These People Operate’: Fmr CIA Officer Calls BS On FBI’s New Epstein Intel
-
 Economy1 day ago
Economy1 day agoThe stars are aligning for a new pipeline to the West Coast
-
 Red Deer1 day ago
Red Deer1 day agoJoin SPARC in spreading kindness by July 14th