COVID-19
Shocking new study shows COVID patients had higher mortality risk if they were vaxxed

From LifeSiteNews
Hospitalized COVID patients who took the jab had a 70% mortality risk compared to 37% for those who did not, according to a new study published by Frontiers in Immunology.
Hospitalized COVID patients have a significantly higher risk of death if they have received a COVID-19 shot, according to a shocking new study published by the journal Frontiers in Immunology.
The study, which examined 152 adult patients who were admitted to the hospital at Ohio State University, and found that “[a]mong COVID-19 patients, mortality rate was significantly higher among Vax vs. NVax [vaccinated vs. not vaccinated] patients,” specifically “70% compared with 37%.”
While those who chose the jab were somewhat more likely to have other comorbidities, the discrepancy remained even “when we compared COVID-19 Vax vs. NVax patients with similar CCI score, suggesting that additional factors may increase risk of mortality,” referring to the Charlson’s Comorbidity Index, which accounts for numerous variables increasing one’s odds of death. The authors said their findings “sugges[t] there are other risk factors in vaccinated patients.”
“As a possible explanation for this observation, recent studies have shown that mRNA (but not vector-based) vaccine-associated increases in SARS-CoV-2 S-specific IgG4 levels vaccines did not contribute to increased protection,” the paper says. “In contrast, they were thought to suppress antiviral immune responses, promoting immune tolerance and, possibly, unrestricted SARS-CoV-2 replication.”
The authors note that their findings are “limited to patients with severe infection admitted to the OSU hospital.”
Overall, the findings contribute to a significant body of evidence associating significant risks with the COVID jabs, which were developed and reviewed in a fraction of the time vaccines usually take under former President Donald Trump’s Operation Warp Speed initiative.
The federal Vaccine Adverse Event Reporting System (VAERS) reports 37,231 deaths, 214,906 hospitalizations, 21,524 heart attacks, and 28,214 myocarditis and pericarditis cases as of February 23, among other ailments. An April 2022 study out of Israel indicates that COVID infection itself cannot fully account for the myocarditis numbers, despite common insistence to the contrary. VAERS reports are technically unconfirmed, as anyone can submit one, but U.S. Centers for Disease Control and Prevention (CDC) researchers have recognized a “high verification rate of reports of myocarditis to VAERS after mRNA-based COVID-19 vaccination,” leading to the conclusion that “under-reporting is more likely” than overreporting.
A 2010 report submitted to the U.S. Department of Health and Human Services’ (HHS’s) Agency for Healthcare Research and Quality (AHRQ) warned that VAERS caught “fewer than 1% of vaccine adverse events.” On the problem of underreporting, the VAERS website offers only that “more serious and unexpected medical events are probably more likely to be reported than minor ones” (emphasis added).
In 2021, Project Veritas shed light on some of the reasons for such underreporting with undercover video from inside Phoenix Indian Medical Center, a facility run under HHS’s Indian Health Service program, in which emergency room physician Dr. Maria Gonzales laments that myocarditis cases go unreported “because they want to shove it under the mat,” and nurse Deanna Paris attests to seeing “a lot” of people who “got sick from the side effects” of the COVID shots, but “nobody” is reporting them to VAERS “because it takes over a half hour to write the d–n thing.”
Further, VAERS is not the only data source containing red flags. Data from the Pentagon’s Defense Medical Epidemiology Database (DMED) shows that 2021 saw drastic spikes in a variety of diagnoses for serious medical issues over the previous five-year average, including hypertension (2,181%), neurological disorders (1,048%), multiple sclerosis (680%), Guillain-Barre syndrome (551%), breast cancer, (487%), female infertility (472%), pulmonary embolism (468%), migraines (452%), ovarian dysfunction (437%), testicular cancer (369%), and tachycardia (302%).
Last September, the Japanese Society for Vaccinology published a peer-reviewed study conducted by researchers from Stanford, UCLA, and the University of Maryland, which found that the “Pfizer trial exhibited a 36% higher risk of serious adverse events in the vaccine group” while the “Moderna trial exhibited a 6% higher risk of serious adverse events in the vaccine group,” for a combined “16% higher risk of serious adverse events in mRNA vaccine recipients.”
In December 2022, U.S. Sen. Ron Johnson (R-WI) hosted a roundtable discussion during which civil rights attorney Aaron Siri detailed data from the CDC’s V-Safe reporting system revealing that 800,000 of the system’s 10 million participants, or approximately 7.7 percent, reported needing medical care after COVID injection. “Twenty-five percent of those people needed emergency care or were hospitalized, and another 48 percent sought urgent care,” Siri added. “Also, another 25 percent on top of the 7.7 percent reported being unable to work or go to school.”
Another study by a team of American, British, and Canadian researchers, published last December in the Journal of Medical Ethics, found that COVID booster mandates for university students – a relatively healthy group at relatively low risk from the virus – do far more harm than good: “per COVID-19 hospitalisation prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines, including 1.5–4.6 booster-associated myopericarditis cases in males (typically requiring hospitalisation).”
Most recently, an analysis of 99 million people across eight countries published in February in the journal Vaccine – the largest analysis to date – “observed significantly higher risks of myocarditis following the first, second and third doses” of mRNA-based COVID shots, as well as signs of increased risk of “pericarditis, Guillain-Barré syndrome, and cerebral venous sinus thrombosis,” and other “potential safety signals that require further investigation.”

 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
As millions of Americans anxiously await action from the new HHS leadership against the COVID-19 mRNA injections—injected into over 9 million children this year—Robert F. Kennedy Jr. has finally gone publicly on the offensive:
Let’s go over each key point made by RFK Jr.:
The recommendation for children was always dubious. It was dubious because kids had almost no risk for COVID-19. Certain kids that had very profound morbidities may have a slight risk. Most kids don’t.
In the largest review to date on myocarditis following SARS-CoV-2 infection vs. COVID-19 vaccination, Mead et al found that vaccine-induced myocarditis is not only significantly more common but also more severe—particularly in children and young males. Our findings make clear that the risks of the shots overwhelmingly outweigh any theoretical benefit:
 |
The OpenSAFELY study included more than 1 million adolescents and children and found that myocarditis was documented ONLY in COVID-19 vaccinated groups and NOT after COVID-19 infection. There were NO COVID-19-related deaths in any group. A&E attendance and unplanned hospitalization were higher after first vaccination compared to unvaccinated groups:
So why are we giving this to tens of millions of kids when the vaccine itself does have profound risk? We’ve seen huge associations of myocarditis and pericarditis with strokes, with other injuries, with neurological injuries.
The two largest COVID-19 vaccine safety studies ever conducted, involving 99 million (Faksova et al) and 85 million people (Raheleh et al), confirm RFK Jr.’s concerns, documenting significantly increased risks of serious adverse events following vaccination, including:
- Myocarditis (+510% after second dose)
- Acute Disseminated Encephalomyelitis (+278% after first dose)
- Cerebral Venous Sinus Thrombosis (+223% after first dose)
- Guillain-Barré Syndrome (+149% after first dose)
- Heart Attack (+286% after second dose)
- Stroke (+240% after first dose)
- Coronary Artery Disease (+244% after second dose)
- Cardiac Arrhythmia (+199% after first dose)
 |
And this was clear even in the clinical data that came out of Pfizer. There were actually more deaths. There were about 23% more deaths in the vaccine group than the placebo group. We need to ask questions and we need to consult with parents.
Actually, according to the Pfizer’s clinical trial data, there were 43% more deaths in the vaccine group compared to the placebo group when post-unblinding deaths are included:
 |
We need to give people informed consent, and we shouldn’t be making recommendations that are not good for the population.
Public acknowledgment of the grave harms of COVID-19 vaccines signals that real action is right around the corner. However, we must hope that action is taken for ALL age groups, as no one is spared from their life-reducing effects:
Alessandria et al (n=290,727, age > 10 years): People vaccinated with 2 doses lost 37% of life expectancy compared to the unvaccinated population during follow-up.
 |
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.


 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
45.3% of “COVID-19 deaths” in Greece had no symptoms — exposing the coordinated PSYOP deployed to maximize fear and enforce mass compliance with draconian control measures.
The study titled “Deaths “due to” COVID-19 and deaths “with” COVID-19 during the Omicron variant surge, among hospitalized patients in seven tertiary-care hospitals, Athens, Greece” was just published in the journal Scientific Reports:
Abstract
In Greek hospitals, all deaths with a positive SARS-CoV-2 test are counted as COVID-19 deaths. Our aim was to investigate whether COVID-19 was the primary cause of death, a contributing cause of death or not-related to death amongst patients who died in hospitals during the Omicron surge and were registered as COVID-19 deaths. Additionally, we aimed to analyze the factors associated with the classification of these deaths. We retrospectively re-viewed all in-hospital deaths, that were reported as COVID-19 deaths, in 7 hospitals, serving Athens, Greece, from January 1, 2022, until August 31, 2022. We retrieved clinical and laboratory data from patient records. Each death reported as COVID-19 death was characterized as: (A) death “due to” COVID-19, or (B) death “with” COVID-19. We reviewed 530 in-hospital deaths, classified as COVID-19 deaths (52.4% males; mean age 81.7 ± 11.1 years). We categorized 290 (54.7%) deaths as attributable or related to COVID-19 and in 240 (45.3%) deaths unrelated to COVID-19. In multivariable analysis The two groups differed significantly in age (83.6 ± 9.8 vs. 79.9 ± 11.8, p = 0.016), immunosuppression history (11% vs. 18.8%, p = 0.027), history of liver disease (1.4% vs. 8.4%, p = 0.047) and the presence of COVID-19 symptoms (p < 0.001). Hospital stay was greater in persons dying from non-COVID-19 related causes. Among 530 in-hospital deaths, registered as COVID-19 deaths, in seven hospitals in Athens during the Omicron wave, 240 (45.28%) were reassessed as not directly attributable to COVID-19. Accuracy in defining the cause of death during the COVID-19 pandemic is of paramount importance for surveillance and intervention purposes.
 |
Key Findings:
Massive Overcounting of COVID-19 Deaths
- Out of 530 hospital deaths registered as COVID-19 deaths, only 290 (54.7%) were actually caused by COVID-19.
- 240 deaths (45.3%) were found to be completely unrelated to COVID-19 — patients died with a positive PCR test, but showed no symptoms, required no COVID-specific treatment, and died of clearly unrelated causes.
Death Certificate Inaccuracy
- Of the 204 certificates listing COVID-19 as the direct cause of death, only 132 (64.7%) were confirmed as such after clinical review.
- Of the 324 certificates listing COVID-19 as a contributing factor, only 86 (26.5%) were found to be truly related.
Hospital-Acquired Infections Misclassified
- Patients infected during hospitalization were significantly more likely to be misclassified as COVID-19 deaths (OR: 2.3, p = 0.001).
Younger Age and Severe Comorbidities Associated with Misclassification
- Patients who died “with” COVID-19 were younger, more likely to be immunosuppressed, have end-stage liver disease, or be admitted for other causes.
Symptoms and Treatments Differed Sharply
Patients who died “due to” COVID-19 were more likely to:
- Exhibit classic symptoms: hypoxia (44.1%), shortness of breath, fever, and cough
- Require oxygen support (93.4% vs. 66.9%) and receive COVID-specific therapies:
- Remdesivir (5-day course: 61.9% vs. 35.2%)
- Dexamethasone (81.7% vs. 40.7%)
Study Strengths
This study went far beyond death certificate coding, implementing a rigorous, multi-source clinical audit:
- Full medical chart reviews: Included physician notes, lab data, imaging, and treatment records.
- Attending physician interviews: Structured questionnaires captured real-time clinical insights from those who treated the patients.
- Dual independent expert assessments: Two experienced infectious disease specialists (each with >2,500 COVID cases) reviewed each case independently for classification accuracy.
This study found that nearly half of all registered COVID-19 deaths during the Omicron wave in Greece were misclassified, with no clinical evidence linking them to COVID-19 as the true cause. Given that similar death coding practices were employed across Western nations, it is reasonable to conclude that COVID-19 death counts were artificially inflated to a comparable degree elsewhere.
This drastic inflation of death counts aligns with what many now understand to be a coordinated psychological operation (PSYOP)—designed to instill fear and maximize compliance with draconian pandemic measures such as lockdowns, mask mandates, and mass mRNA injection campaigns.
It is this weaponization of fear that has prompted criminal referrals in seven U.S. states, triggering active criminal investigations into top COVID-19 officials for terrorism, murder and racketeering:
BREAKING – The Pandemic Justice Phase Begins as Criminal Investigations Commence |
||||||
|
||||||
 |
||||||
|
By Nicolas Hulscher, MPH
|
||||||
|
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.



Province to expand services provided by Alberta Sheriffs: New policing option for municipalities

Made in Alberta! Province makes it easier to support local products with Buy Local program
Is HNIC Ready For The Winnipeg Jets To Be Canada’s Heroes?

CSIS Warned Beijing Would Brand Conservatives as Trumpian. Now Carney’s Campaign Is Doing It.
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoOttawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoBREAKING: THE FEDERAL BRIEF THAT SHOULD SINK CARNEY
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoHow Canada’s Mainstream Media Lost the Public Trust
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoReal Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoCHINESE ELECTION THREAT WARNING: Conservative Candidate Joe Tay Paused Public Campaign
-
COVID-191 day ago
Nearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal
-
 John Stossel1 day ago
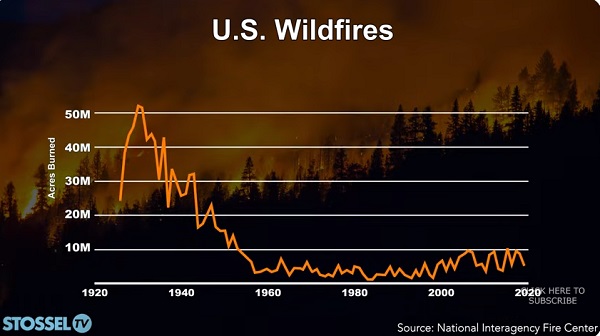
John Stossel1 day agoClimate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
 Media23 hours ago
Media23 hours agoCBC retracts false claims about residential schools after accusing Rebel News of ‘misinformation’