COVID-19
Nurse testimonials reveal ‘perfect storm’ of hospital COVID protocols leading to patient death

From LifeSiteNews
Hospitals were given money bonuses to enact dangerous protocols on COVID patients, according to whistleblower nurses who were themselves punished for speaking out.
Nurse testimonials reveal that hospitals not only used a deadly cocktail of protocols facilitating the death of patients during the COVID outbreak but punished whistleblowers, an author and researcher recently explained.
COVID policymakers “created one of the biggest terror campaigns in the history of mankind,” Ken McCarthy told Polly Tommey of Children’s Health Defense last month while sharing the most shocking findings of his tell-all interviews with nurses who worked the COVID pandemic.
McCarthy told how when he began to speak with nurses about their experiences, he realized that COVID-era hospital abuses he knew were taking place in New York City were in fact taking place nationwide due to “top down driven” protocols from the National Institutes of Health (NIH).
These protocols, McCarthy said, were being “filtered through” chief financial officers (CFOs) of hospitals, because they were being “heavily” financially incentivized. And they were, according to all that he had learned from the nurses, dangerous and even deadly to those were designated COVID patients.
McCarthy went down the line naming several incentivized hospital COVID protocols that inflicted harm on these patients, beginning with the denial of anti-inflammatories like ibuprofen, as well as inhalable steroids.
“That’s the normal way you treat respiratory distress. You knock the inflammation down and you give people steroids. If you had a positive COVID diagnosis, they wouldn’t give you those basic treatments. This is like a fireman showing up at the fire and saying, let it burn a little bit more before we do anything,” McCarthy shared.
The next harmful practice hospitals used on “COVID” patients was to strap BiPAP masks on patients, a form of non-invasive ventilation that when administered improperly, caused many patients to have panic attacks.
“When you treat somebody with that, you have to warn them … It’s like if you were driving at 80 miles an hour and then one of your passengers stuck their head out the window. The wind is going down that fast. They didn’t prepare the patients, they didn’t comfort the patients. They would just slap this thing on and leave them alone,” explained McCarthy, adding that this “understandably” triggered panic attacks, at which point they were offered tranquilizers.
These tranquilizers relaxed their muscles, including their diaphragm, thereby weakening their breathing.
On top of all of this, hospitals were financially rewarded for administering the “failed drug” Remdesivir to COVID patients, the use of which McCarthy noted was halted in Africa where it was used for Ebola, because it caused organ failure.
The drug was also dropped from a clinical trial for Ebola in 2018 after it was found that it had the highest death rate of the four drugs being tested, Dr. Bryan Ardis shared in a 2021 interview. In addition, according to attorney Thomas Renz, 25.9% of those prescribed Remdesivir for COVID-19 are recorded as having died in the Centers for Medicare & Medicaid Services (CMS) database. The death rate for COVID patients prescribed Remdesivir dwarfs the fatality rate of COVID patients prescribed Ivermectin, which is recorded by the CMS database as being 7.2%.
The deadly clincher to these protocols was the invasive intubation, that is, the use of ventilators, which were also financially incentivized.
McCarthy told Tommey that such intubation is for “when you’ve exhausted every other possibility” for a patient, because it is “a dangerous procedure.”
“The nickname for it among the hospital people is the garden hose. It’s large. Then you have to give somebody a feeding tube … You can cause abrasions, you can cause bleeding, infections.”
McCarthy learned that, moreover, intubated patients are typically given anywhere from five to 15 different drugs, including analgesics like fentanyl needed for the severe pain of invasive intubation, paralytic agents, and drugs “to just knock you out.”
He explained that normally a respiratory therapy is supposed to watch over four or five intubated patients, whereas during COVID, there was typically only one such therapist “for an entire ward of people.”
“Recipe for disaster. And indeed there was disaster,” McCarthy said.
“Now, here’s the really sinister thing. If you kept (a patient) on for 90 hours or longer, you got an extra bonus,” he continued.
“Every respiratory therapist will tell you as soon as you intubate somebody, within 24 hours you’re testing to see, hey, has this person recovered enough that we can take them off the intubation? Because every day you’re on intubation, you are closer to death. That’s just a fact.”
“So by what stretch of insanity did they incentivize hospitals to keep people on for 90 hours?” said McCarthy, adding, “I’d love to know who was in that room planning out these protocols.”
The author stressed that hospitals nowadays act as corporations, and not charitable institutions like they used to be — that is, they are “bottom line people.” So when they are given money bonuses for enacting certain protocols, they simply direct their entire staff to carry them out.
McCarthy said that in order to hide these deadly protocols, hospitals punished whistleblowers, according to nurse testimony.
A group that “was literally affiliated with the United Nations,” Team Halo, who McCarthy noted was devoted to counteracting “anti-vaxxers,” “metamorphized” during the COVID outbreak into a group that went after whistleblower nurses.
“They gave out nurses’ addresses and telephone numbers. They encouraged unhinged people to show up at their door and threaten them,” said McCarthy, telling how one whistleblower nurse who lives “in the boondocks of Nevada” had people “showing up at her door” after she was doxxed.
“They also had people filing complaints against the nurses with the nursing boards. Many of them had their nursing licenses challenged,” McCarthy added.
“And these were the thugs that went out and terrorized these nurses. So not only did the nurses get abused on the job — they were all fired. Anybody that spoke up and wouldn’t stop speaking up was fired. They were also tracked down afterwards and punished. They went through hell,” McCarthy said.
McCarthy’s book about his findings, “What the Nurses Saw,” is currently being sold on Amazon and has garnered an average of full five-star reviews.


|
A Canadian court has ordered the release of documents that could shed light on how federal authorities and law enforcement worked together to freeze the bank accounts of a protester involved in the Freedom Convoy.
Both the RCMP and TD Bank are now required to provide records related to Evan Blackman, who took part in the 2022 demonstrations and had his accounts frozen despite not being convicted of any crime at the time.
The Justice Centre for Constitutional Freedoms (JCCF) announced the Ontario Court of Justice ruling. The organization is representing Blackman, whose legal team argues that the actions taken against him amounted to a serious abuse of power.
“The freezing of Mr. Blackman’s bank accounts was an extreme overreach on the part of the police and the federal government,” said his lawyer, Chris Fleury. “These records will hopefully reveal exactly how and why Mr. Blackman’s accounts [were] frozen.”
Blackman was arrested during the mass protests in Ottawa, which drew thousands of Canadians opposed to vaccine mandates and other pandemic-era restrictions.
Although he faced charges of mischief and obstructing police, those charges were dismissed in October due to a lack of evidence. Despite this, prosecutors have appealed, and a trial is set to begin on August 14.
At the height of the protests, TD Bank froze three of Blackman’s accounts following government orders issued under the Emergencies Act. Then-Prime Minister Justin Trudeau had invoked the act to grant his government broad powers to disrupt the protest movement, including the unprecedented use of financial institutions to penalize individuals for their support or participation.
In 2024, a Federal Court Justice ruled that Trudeau’s decision to invoke the act had not been justified.
Blackman’s legal team plans to use the newly released records to demonstrate the extent of government intrusion into personal freedoms.
According to the JCCF, this case may be the first in Canada where a criminal trial includes a Charter challenge over the freezing of personal bank accounts under emergency legislation.
|

From LifeSiteNews
Pfizer and Moderna’s mRNA COVID shots must now include warnings that they cause ‘extremely high risk’ of heart inflammation and irreversible damage in males up to age 24.
The Trump administration’s Food and Drug Administration (FDA) announced it will now require updated safety warnings on mRNA COVID-19 shots to include the “extremely high risk” of myocarditis/pericarditis and the likelihood of long-term, irreversible heart damage for teen boys and young men up to age 24.
The required safety updates apply to Comirnaty, the mRNA COVID shot manufactured by Pfizer Inc., and Spikevax, the mRNA COVID shot manufactured ModernaTX, Inc.
According to a press release, the FDA now requires each of those manufacturers to update the warning about the risks of myocarditis and pericarditis to include information about:
- the estimated unadjusted incidence of myocarditis and/or pericarditis following administration of the 2023-2024 Formula of mRNA COVID-19 shots and
- the results of a study that collected information on cardiac magnetic resonance imaging (cardiac MRI) in people who developed myocarditis after receiving an mRNA COVID-19 injection.
The FDA has also required the manufacturers to describe the new safety information in the adverse reactions section of the prescribing information and in the information for recipients and caregivers.
Additionally, the fact sheets for healthcare providers and for recipients and caregivers for Moderna COVID-19 shot and Pfizer-BioNTech COVID-19 shot, which are authorized for emergency use in individuals 6 months through 11 years of age, have also been updated to include the new safety information in alignment with the Comirnaty and Spikevax prescribing information and information for recipients and caregivers.
In a video published on social media, Dr. Vinay Prasad, director of the Center for Biologics Evaluation & Research Chief Medical and Scientific Officer, explained the alarming reasons for the warning updates.
While heart problems arose in approximately 8 out of 1 million persons ages 6 months to 64 years following reception of the cited shots, that number more than triples to 27 per million for males ages 12 to 24.
Prasad noted that multiple studies have arrived at similar findings.



RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
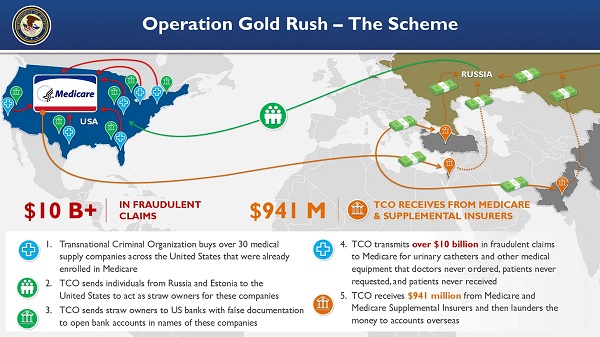
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Fraser Institute1 day ago
Fraser Institute1 day agoBefore Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually
-
 Crime2 days ago
Crime2 days ago“This is a total fucking disaster”
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV
-
 Daily Caller2 days ago
Daily Caller2 days ago‘I Know How These People Operate’: Fmr CIA Officer Calls BS On FBI’s New Epstein Intel
-
 MAiD2 days ago
MAiD2 days agoCanada’s euthanasia regime is already killing the disabled. It’s about to get worse
-
 Daily Caller2 days ago
Daily Caller2 days agoBlackouts Coming If America Continues With Biden-Era Green Frenzy, Trump Admin Warns
-
 Red Deer2 days ago
Red Deer2 days agoJoin SPARC in spreading kindness by July 14th
-
 Business1 day ago
Business1 day agoPrime minister can make good on campaign promise by reforming Canada Health Act