COVID-19
My kid has covid. Now what do we do? – Dr. Peter McCullough Interview Part 2

This may seem a little strange because I’m going to willingly breech my own doctor / patient confidentiality. I’m not sure what my obligation is here but I know doctors are guided by the Health Information Act (HIA) and the Personal Information Protection Act (PIPA). Nowadays though we all know that every time I go to coach my son’s hockey team I have to divulge my health information in front of whoever happens to be near me in front of a stranger in the entrance of a hockey rink. In other words, I’m guessing I’ll get away with this.
Recently I asked my doctor the same question we all should be asking our doctors. “If I get a positive covid result and I’m symptomatic, can I call you and ask for some kind of treatment?”
My doctor answered in the way I suspect most doctors would. He looked at me quizzically and said “You mean in hospital? You’ll be treated by the doctors there.”
That’s not what I meant and I said, “No. I mean if I have symptoms. Will you offer me treatment to help me stay ‘out’ of the hospital in the first place?”
My doctor is a pretty good egg and I like him and all but from his response I know that if (when) I get covid I am going to be in the same position as almost every other Albertan. I will go home and isolate and pray that this doesn’t get serious.
I don’t know about you, but as far as I’m concerned that doesn’t seem good enough. I’d like to think there are treatments out there and maybe that’s why I really like to research articles with data regarding Ivermectin and Hydroxychloroquine (not to mention Zinc and vitamins D, and C). Months ago these were just stories. Then I started to meet people who told me about a family member or friend who quickly bounced back after taking treatment for covid. Then I met a couple of those people myself. Now I’m convinced there’s something to all these articles I’m reading.

The studies say (so does my experience with people I know) that these treatments don’t work every time. However, if you could save even 10 percent of lives and keep even 10 percent of people out of the hospital by taking an inexpensive drug that has no serious side effects, why wouldn’t you promote the living (beep) out of that? Seriously? What if it was 20 or 30 or 50%. It’s incredible to me that so many people will turn their noses at something like Ivermectin because someone on TV called it ‘horse dewormer’. For my opinion of the people who block their ears and yell “HORSE DEWORMER” see here. If you’ve been doing that, please stop. I guarantee you someone you know and maybe even love has either taken Ivermectin, or they’re going to want to some day. You may not know there are actually quiet a few studies. Maybe you haven’t met anyone who swears they turned around within hours of getting treatment. But trust me, the people making decisions for us (the politicians at the very top and even more importantly the health officials) know there are treatments out there. They’ve just chosen not to pursue them.
While those who supposedly follow the science denounce studies that looked extremely promising but were really too small, or studies that were done so far away that we simply don’t know enough to give them credence, other people who also supposedly follow the science have found some very interesting data themselves. Just check out this beauty from the American Journal of Therapeutics, called Ivermectin for Prevention and Treatment of COVID-19 Infection, published back on June 21 of 2021. This is way better than 10%. This looks really promising. This is also being completely ignored by our political leaders. Don’t ask me why. Seriously don’t ask unless you have at least 2 tall boys.
The bottom line is, after all I’ve read and seen and the people I’ve met, I refuse to believe there is no such thing as a treatment for covid. I know they’re coming out with new ones for this specific purpose, but I’m convinced by data that there are repurposed drugs that are already doing the job. Not perfectly of course, but far better than say .. nothing.
This really gets me when I think about my children. The thought of one of my kids getting covid and then becoming symptomatic, and then getting really ill, and then not being able to access treatment when I’m pretty sure there’s something out there that would help them… That’s not a very nice thought. It became real for me recently when a good friend told me his son (same age as my son) tested positive. He knows I’m keeping up on this as much as I can and he texted to let me know (and I think ask if I could recall some of the things I’ve said to him about treatment). I shared the video I’m sharing here, below. I also emailed links to two very similar resources for us regular folks who can only talk about the people who actually follow the science. I’ll include these links because I think they’re REALLY worth looking at. Especially because there’s literally nothing else to look at when someone in your household gets a positive test result. Here’s the Guide to Home Based Treatment for Covid from the American Association of Physicians and Surgeons, and here’s the Guide to Covid Early Treatment from a group of US doctors on their website TruthForHealth.
The video below refers only to children but the two “home treatment” guides are helpful for people at any age. I hope you never need this kind of info, but personally I don’t think we’re going to achieve the magical zero covid even if we take all the vaccine in the world. This very nasty virus is here to stay. The way we’re going to get back to living like we should be, is with EARLY treatment.. as in BEFORE we’re deathly ill in the hospital. I suspect we’re about 6 months away from recognized and emergency approved early treatment pills that will eventually swoop in and save the day for the vast majority. But seriously, who cares if you put out a fire with water, or retardant, or a cut line, or by stomping on it with your foot? The important thing is that you start fighting fire as soon as you can. For me? I’m happy to start by throwing a little dirt on this campfire while I wait for the water bombers.
Thanks for checking this out. If you need a bit more convincing that early treatment even exists.. check out this next article.

From LifeSiteNews
Lawyers will argue that there is no evidence linking Tamara Lich ‘to the misdeeds of others.’
Freedom Convoy leader Tamara Lich said she will appeal her recent mischief conviction in an Ontario court, with her lawyers saying “there was no evidence linking her to the misdeeds of others.”
In a press release late yesterday, Lich’s legal team, headed by Lawrence Greenspon, Eric Granger, and Hannah Drennan, made the announcement.
“Lawyers for Tamara Lich filed Notice of Appeal in the Ontario Court of Appeal of the conviction for mischief arising out of the Freedom Convoy,” the release stated.
Lich’s legal team noted that there are two reasons for the principal grounds of appeal.
“While there was substantial evidence that Tamara encouraged the protesters to be peaceful, lawful and safe, there was no evidence linking her to the misdeeds of others,” they said.
The second reason for the appeal, according to Lich’s lawyers, is that the “trial judge failed to give effect to the principle that communication that would otherwise be mischief is protected by section 2(b) of the Charter, freedom of expression.”
On October 7, Ontario Court Justice Heather Perkins-McVey sentenced Lich and Chris Barber to 18 months’ house arrest after being convicted earlier in the year of “mischief.”
Lich was given 18 months less time already spent in custody, amounting to 15 1/2 months.
As reported by LifeSiteNews, the Canadian government was hoping to put Lich in jail for no less than seven years and Barber for eight years for their roles in the 2022 protests against COVID mandates.
Interestingly, Perkins-McVey said about Lich and Barber during the sentencing, “They came with the noblest of intent and did not advocate for violence.”
As reported by LifeSiteNews, Lich, reflecting on her recent sentencing of over a year’s house arrest for her role in the 2022 Freedom Convoy, laid bare the fact that when all is said in done, seven years of her life will have been spent in a government-imposed “lockdown” in one form or another.
LifeSiteNews recently reported that Lich detailed her restrictive house arrest conditions, revealing she is “not” able to leave her house or even pick up her grandkids from school without permission from the state.
As reported by LifeSiteNews, Lich, reflecting on her recent house arrest verdict, said she has no “remorse” and will not “apologize” for leading a movement that demanded an end to all COVID mandates.

From LifeSiteNews
When the convoy first came to Ottawa, allegations were floated that the memorial had been desecrated. After learning of this, Evely quickly organized a group of veterans to stand guard around the clock to protect the area.
A Canadian veteran appealed to the Ontario courts after he was convicted for organizing a guard around the National War Memorial during the Freedom Convoy.
In an October press release, the Justice Centre for Constitutional Freedoms (JCCF) announced that an appeal has been filed in the Ontario Court of Appeals on behalf of Master Warrant Officer (Ret’d) Jeffrey Evely over his conviction for mischief and obstructing police while on his way to guard the Ottawa War Memorial during the 2022 Freedom Convoy.
“By locking down large sections of downtown Ottawa, the police were effectively preventing all civilians from accessing public areas and greatly exceeded their powers under the common law,” constitutional lawyer Chris Fleury explained.
“This case raises issues that have implications for protests across the province and the country. We are hopeful that the Ontario Court of Appeal will agree and grant leave to appeal,” he added.
The appeal argues that police overstepped their authority in their response to the 2022 protest of COVID mandates. Police actions at the time included locking down the Ottawa core, establishing checkpoints, and arresting protesters.
In September 2024, Everly was convicted of mischief and obstruction after his involvement in the 2022 Freedom Convoy, which protested COVID mandates by gathering Canadians in front of Parliament in Ottawa.
As LifeSiteNews previously reported, when the convoy first came to Ottawa, allegations were floated that the memorial had been desecrated. After learning of this, Evely quickly organized a group of veterans to stand guard around the clock to protect the area.
However, under former Prime Minister Justin Trudeau’s use of the Emergencies Act, many parts of downtown Ottawa were blocked to the public, and a vigilant police force roamed the streets.
It was during this time that Evely was arrested for entering a closed off section of downtown Ottawa during the early hours of February 19, 2022. He had been on his way to take the 4:25 a.m. shift protecting the Ottawa War Memorial.
As Evely walked to the memorial, he was allegedly told to stop by police. According to the police, Evely “ran for a short distance before being confronted by two additional police officers.”
He was forcibly pushed to the ground, landing face first. The veteran was then arrested and charged with mischief and obstructing police.
At the time, the use of the EA was justified by claims that the protest was “violent,” a claim that has still gone unsubstantiated.
In fact, videos of the protest against COVID regulations and shot mandates show Canadians from across the country gathering outside Parliament engaged in dancing, street hockey, and other family-friendly activities.
Indeed, the only acts of violence caught on video were carried out against the protesters after the Trudeau government directed police to end the protest. One such video showed an elderly women being trampled by a police horse.
While the officers’ actions were originally sanctioned under the EA, Federal Court Justice Richard Mosley ruled that Trudeau was “not justified” in invoking the EA, forcing Crown prosecutors to adopt a different strategy.
Now, Crown prosecutors allege that the common law granted police the authority to stop and detain Evely, regardless of the EA.
However, Evely and his lawyers have challenged this argument under section 9 of the Canadian Charter of Rights and Freedoms, insisting that his “arrest and detention were arbitrary.”
Earlier this month, Freedom Convoy organizers Tamara Lich and Chris Barber were sentenced to 18-month house arrest after a harrowing 25-month trial process. Many have condemned the sentence, warning it amounts to “political persecution” of those who stand up to the Liberal government.

Trans Mountain executive says it’s time to fix the system, expand access, and think like a nation builder
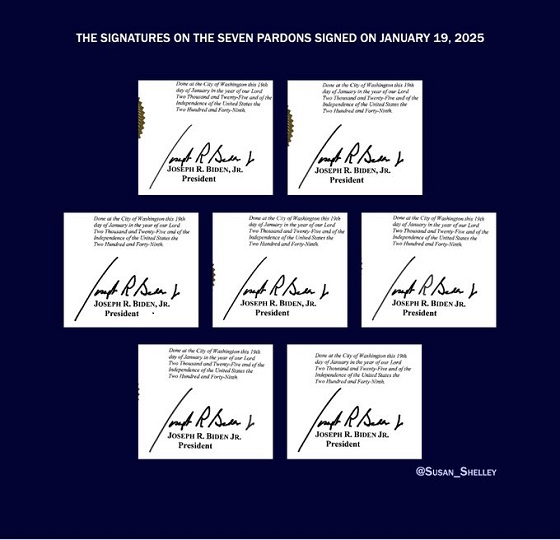
Biden’s Autopen Orders declared “null and void”

Study promotes liver transplants from Canadian euthanasia victims

Musk launches Grokipedia to break Wikipedia’s information monopoly

-
 Business2 days ago
Business2 days agoBudget 2025 continues to balloon spending and debt
-
 Censorship Industrial Complex2 days ago
Censorship Industrial Complex2 days agoHow the UK and Canada Are Leading the West’s Descent into Digital Authoritarianism
-
 Business2 days ago
Business2 days agoFederal budget: Carney government posts largest deficit in Canadian history outside pandemic
-
 Business2 days ago
Business2 days agoCapital Flight Signals No Confidence In Carney’s Agenda
-
 Economy2 days ago
Economy2 days agoThe True Cost of Mark Carney’s Ineffective Green Energy Sinkhole
-
 International2 days ago
International2 days agoThe capital of capitalism elects a socialist mayor
-
 Daily Caller1 day ago
Daily Caller1 day agoUS Eating Canada’s Lunch While Liberals Stall – Trump Admin Announces Record-Shattering Energy Report
-
 Business1 day ago
Business1 day agoPulling back the curtain on the Carney government’s first budget