David Clinton
Is Canada Abusing the Charter of Rights and Freedoms?



Canadians have no absolute right to equal treatment under the law.
Monitoring the intersection between equality and equity
Let me explain that. Section 15 of the Charter of Rights and Freedoms was, from the perspective of the Charter’s creators, an exceedingly difficult needle to thread. The tension between its two subsections carries the potential for confusion and even abuse. Here’s the text itself:
(1) Every individual is equal before and under the law and has the right to the equal protection and equal benefit of the law without discrimination and, in particular, without discrimination based on race, national or ethnic origin, colour, religion, sex, age or mental or physical disability.
(2) Section (1) does not preclude any law, program or activity that has as its object the amelioration of conditions of disadvantaged individuals or groups including those that are disadvantaged because of race, national or ethnic origin, colour, religion, sex, age or mental or physical disability.
15(1) guaranteed the equal treatment of all individuals. That’s something I can’t imagine any reasonable-minded person opposing. The problem was that, at the same time, the authors also wanted to leave room for unfair treatment for select groups through affirmative action programs. That’s the purpose of 15(2).
The Audit is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
If 15(2) didn’t exist, challenges to, say, hiring practices targeting historically disadvantaged racial groups could be launched based on the rights found in 15(1). Imagine people who didn’t technically qualify as disadvantaged but who might be better suited for and in greater immediate need of an advertised job. If the “affirmative action” candidate was nevertheless hired, couldn’t the others argue that they’d just suffered Charter-level discrimination? 15(2) is designed to ensure such challenges don’t happen.
Such state-imposed inequality may or may not be justifiable. That’s a debate that doesn’t interest me right now. Instead, my primary focus is on how the principle could be widely abused.
I should clarify that these rules only apply to government programs and agencies. While private companies might be bound by other areas of related law, the Charter was only written for government operations. But it’s nevertheless worth remembering that 4.4 million Canadians work for one level or another of government (when you include hospitals and public schools). That’s around 21 percent of all Canadian workers. And many more of us interact with governments regularly.
What kinds of abuse are possible? Well, consider how so many equality-related decisions are highly subjective and rely on the good faith and clarity of mind of the policy makers and public officials in positions of power. In that context:
- How can we know that factors like “ameliorative”, “disproportionate”, or “disadvantaged” are accurately and appropriately defined?
- How can we know that favoring one group won’t cause deep and irreparable harm to others?
- How can we know that even good-faith decisions aren’t made based on outdated assumptions or inaccurate stereotypes?
Easy-to-imagine practical examples of abuse could include:
- Provincial scholarship programs that target low-income students from only certain ethnic groups while excluding members of other groups who might currently experience even greater financial hardship.
- Seats in highly competitive university programs that are restricted to only candidates expressing specified identities without objective evidence that such individuals are currently meaningfully underrepresented in those programs or professional fields.
- Government-funded employment programs that subtly target communities likely to share particular political beliefs.
- Internal career advancement policies that prioritize identity and ethnicity over competence that lead to reduced organizational capacity.
- Social disruption due to arbitrary official favoritism for some ethnicities and identities over others.
Of course, misuse of 15(2) can always be tested in court. Programs are, after all, expected to pass the Oakes Test (for objectives that are pressing and substantial) and the Kapp Test (for goals that are truly ameliorative and appropriately targeted).
But that requires someone who notices the problem and has the considerable means necessary to launch a court challenge. There aren’t many people like that running around.
A government that felt that misuse of the law was causing significant damage to society could choose to by-pass 15(2) altogether by invoking the Notwithstanding Clause or by amending the constitution itself. But…well, good luck surviving either attempt.
More realistically, the government could write new legislation that guides the interpretation or application of 15(2). That could mean carefully defining what constitutes an “ameliorative program” or setting clear eligibility criteria for such programs. There would be no need to change the constitution, simply to properly define it.
Alternatively, governments could govern by example. This might mean tailoring their own policies and programs to reflect a more constrained interpretation of 15(2). They could actively participate in court cases to advocate for particular interpretations and present compelling arguments to influence how courts understand and apply the provision.
Finally, of course, they could appoint judges to the Supreme Court and federal courts who are more aligned with values associated with absolute equality under the law.
Subscribe to The Audit.
For the full experience, upgrade your subscription.


To my great surprise I recently noticed that, despite being deeply engaged in wars against at least four determined enemies, Israel doesn’t spend all that much more on their military than Canada does on its forces. What might that tell us about government efficiency?
There’s fairly universal agreement that Canada doesn’t spend enough on its military. But before we can even ask how much we should be spending, we should understand how much we’re already spending. And figuring that out isn’t nearly as easy as I’d expected.
According to the 2025–26 Expenditures by Purpose data released by the Treasury Board Secretariat, the Department of National Defence (DND) was allocated $35.7 billion (CAN). However, the New York Times recently reported that Primer Minister Carney’s $9.3 billion increase would bring the total defence-related spending to $62.7 billion – which suggests that, prior to the increase, we were set to spend $53.4 billion (CAN).
So I’ll work with both of those figures: $35.7 billion ($26 billion USD) and the pre-announcement $53.4 billion ($39 billion USD). By contrast, Israel currently spends around $37 billion (USD) on the Israel Defense Forces (IDF) which is in the neighborhood of 18 percent of their total budget.¹ The IDF is (literally) getting a much bigger bang for their buck.²
I’m going to compare the military inventories of both countries to get a sense of what a dollar of government spending can get you. I understand that this isn’t an apples-to-apples comparison and there are many complicating factors here. But I think the exercise could lead us to some useful insights. First off, here’s a very rough estimate of existing inventories:
 |
I’m sure there are plenty of caveats we could apply to those numbers, including how much of that equipment is actually fit for service on any given day. But they’ll have to do.
In addition, there are currently 68,000 regular troops in the Canadian Armed Forces (CAF) along with 22,500 reserves, while the IDF employs 169,500 regular troops and 465,000 reserves. They also cost money.
Based on some very rough estimates,³ I’d assess the value of IDF assets at around 2.6 times the value of comparable CAF assets. That means that the IDF – using their procurement systems – would need to spend just $14.4 billion (USD) to purchase the equivalent of the current set of CAF assets.
Now compare that with our actual (pre-increase) expenditures of either $26 billion USD or $39 billion USD and it seems that we’re overspending by either 80 percent or 270 percent.
I think we’d be wise to wonder why that is.
For full context, Israel receives around $3.8 billion (USD) in military aid annually from the U.S.
Speaking of which, for simplicity, I completely left the ongoing costs of ordinance out of my calculations.
If you’re really interested, you can see my calculations here.
Subscribe to The Audit.
For the full experience, upgrade your subscription.


 David Clinton
David Clinton
Ontario’s Auditor General just released a performance audit on the Toronto District School Board. I’m sure it’ll surprise exactly no one that “financial and capital resources are not consistently allocated in the most cost-effective or efficient way” or that “The effective management of operations was not always being measured and assessed for internal decision-making”.
And there was plenty of institutional chaos:
“Between 2017/18 and 2022/23…about 38% of TDSB schools did not report conducting the minimum number of fire drills required by the Ontario Fire Code annually, and about 31% of TDSB schools did not report conducting the minimum number of lockdown drills required by TDSB policy annually. The TDSB does not have an effective process to ensure the required number of drills are performed by each school, each year, or that they are performed in accordance with TDSB policy when performed.”
What else would you expect from a massive government bureaucracy that employs 40,000 people, spends $3.6 billion annually and – based on many of the highlighted items on their website – is laser-focused on pretty much anything besides education?
What you might not have seen coming was that around half of the report centered on in-school violence. To be sure, we’re told that there were only 407 violent events reported to the board during the 2022/2023 school year – which is a rate of around 17 events for every 10,000 students. 17:10,000 doesn’t exactly sound like an environment that’s spiraling out of control.
There was a caveat:
“Due to input errors by principals, the TDSB underreported the number of violent incidents that occurred between 2017/18 to 2021/22 to the Ministry by about 9%.”
Ok. But we’re still nowhere near Mad Max levels of violence. So what’s attracting so much of the auditor’s attention? Perhaps it’s got something to do with a couple of recent surveys whose results don’t quite match the board’s own records. Here’s how the audit describes the first of those:
“The 2022/23 TDSB Student and Parent Census was responded to by over 138,000 students, parents, guardians and caregivers. It showed that 23% of students in Grades 4 to 12 that responded to the survey said they were physically bullied (e.g., grabbed, shoved, punched, kicked, tripped, spat at), and about 71% stated they were verbally bullied (e.g., sworn at, threatened, insulted, teased, put down, called names, made fun of). Further, about 14% of student respondents indicated they had been cyberbullied. TDSB’s central tracking of all bullying incidents is much lower than this, suggesting that they are not centrally capturing a large number of bullying incidents that are occurring.”
“23% of students in Grades 4 to 12 that responded to the survey said they were physically bullied”. That’s not a great fit with that 17:10,000 ratio, even if you add the 9 percent of underreported incidents. And bear in mind that these students and their families were willing to discuss their experiences in a survey run by the school board itself, so it’s not like they’re hard to find.
But that’s not the worst of it. The Elementary Teachers’ Federation of Ontario (ETFO) ran their own survey in 2023. They wanted to hear about their members’ experiences with workplace violence. Here, quoting from the audit report, is what TDSB respondents told them:
- 42% had experienced physical force against themselves in 2022/23;
- 18% had experienced more than 10 of these physical force incidents in 2022/23;
- 81% indicated the number of violent incidents increased since they started working;
- about 77% responded that violence was a growing problem at their school;
- about 29% indicated they had suffered a physical injury;
- 57% had suffered a psychological injury/illness (such as mental stress, psychological or emotional harm) as a result of workplace violence against them; and
- about 85% indicated that violence at their school made teaching and working with students more difficult.
29 percent of teachers suffered a physical injury due to workplace violence. That’s elementary school teachers we’re talking about.
For perspective, even accounting for the 9 percent underreporting, the TDSB was aware of events impacting less than a quarter of a percentage point of their students (and apparently didn’t report any violence against teachers). But by their own accounts, 23 percent of all students and 42 percent of elementary teachers have suffered attacks. Are board officials willfully ignoring this stuff?
And if only there was some way to address violence and other criminal activities on school property. Perhaps – and I’m just spitballing here – there could even be people working in schools whose job it would be to (what’s the word I’m looking for?) police crime.
On a completely unrelated note, back in November, 2017, the Toronto District School Board voted 18-3 to permanently end their School Resource Officer (SRO) program. Since then, police officers have been unwelcome on board property.
To be sure, the TDSB has “accepted” all 18 of the report’s recommendations. But talk is cheap. Who’s to say that commitment won’t play out the same way we’ve seen with their fire drill compliance.
Can you spell “class action lawsuit”?


RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
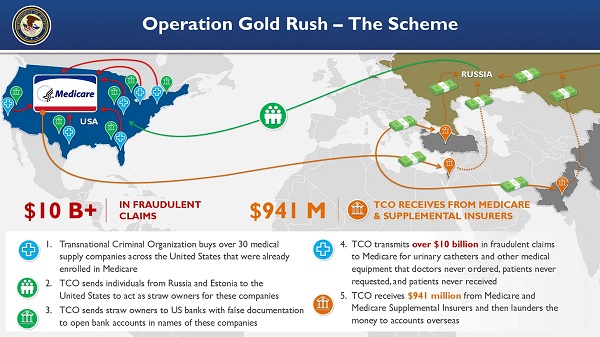
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud

-
 Crime1 day ago
Crime1 day ago“This is a total fucking disaster”
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV
-
 Fraser Institute1 day ago
Fraser Institute1 day agoBefore Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually
-
 Daily Caller2 days ago
Daily Caller2 days agoBlackouts Coming If America Continues With Biden-Era Green Frenzy, Trump Admin Warns
-
 MAiD1 day ago
MAiD1 day agoCanada’s euthanasia regime is already killing the disabled. It’s about to get worse
-
 Daily Caller2 days ago
Daily Caller2 days ago‘I Know How These People Operate’: Fmr CIA Officer Calls BS On FBI’s New Epstein Intel
-
 Business1 day ago
Business1 day agoPrime minister can make good on campaign promise by reforming Canada Health Act
-
 Economy1 day ago
Economy1 day agoThe stars are aligning for a new pipeline to the West Coast