Health
How the Trump-RFK Jr. coalition could realign US politics against Big Pharma and Big Food


From LifeSiteNews
By Jay Richards
If the unlikely coalition of Donald Trump and Robert F. Kennedy Jr. outlives the 2024 presidential election, it could reorder our political categories and leave to our children and grandchildren a quite different future.
When Robert F. Kennedy, Jr. endorsed Donald Trump on Aug. 23, the corporate press and conventional Washington, D.C., analysts mostly missed the real story: It was the moment that a disparate, diverse, and potentially disruptive throng of average Americans became a coalition.
Although RFK, Jr. is famous – or infamous, depending on your view – for his criticisms of vaccines, that wasn’t the theme of his lengthy speech. He spoke instead about an unholy alliance – a cartel – of industries, corporate media, government regulatory agencies, and even nonprofit “charities” that is making us fat and sick. This problem doesn’t fit the simple taxonomy of “public” and “private” or “left” and “right” that served us well during the Cold War.
Kennedy has been a voice in the wilderness warning about this cartel for years. Most Americans first became aware of it during the 2020 pandemic. Here’s the basic story: COVID-19 itself was likely the product of dangerous gain-of-function research conducted by the Wuhan Institute of Virology in China. That’s bad enough. But Communist China didn’t act alone. This work was funded, at least in part, by the U.S. government’s National Institutes of Health and laundered through the nonprofit EcoHealth Alliance.
Once the virus was out, the absurd and counterproductive lockdowns and hygiene theater were pushed by global entities such as the World Health Organization. Domestically, Francis Collins, then-head of the NIH, and Anthony Fauci, then-head of the National Institute of Allergy and Infectious Diseases, worked to undermine independent experts who criticized the federal bureaucrats’ favored policies.
Collins and Fauci even orchestrated the publication of a deceptive article in Nature that claimed the virus had a natural origin. The Centers for Disease Control and Prevention and other federal entities, including the Biden White House, pressured social media platforms to censor even the best-credentialed dissenters.
Attentive Americans soon learned that public health, as a field, focuses on nudging whole populations, rather than seeking the health of individual patients.
Certain pharmaceutical companies – which pay royalties to many NIH staff, including Collins and Fauci – enjoyed a suspiciously fast and less than rigorous approval process for their mRNA “vaccines.” Vaccine mandates then created a massive artificial market for the drugs. And drug companies’ immunity from legal liability allowed them to enjoy the financial benefits of these policies without facing the downside risks from any long-term harm to those who took the vaccines.
Then, during the lockdowns, the growing awareness of the “gender-industrial complex” – media, medical professionals, pharmaceutical companies, politicians, and others who push ghoulish “gender-affirming” interventions on people distressed about their sexed bodies – further reinforced the lack of credibility of private and public health authorities.
An American epidemic of chronic diseases
For some, much of this may now seem obvious. What may be less obvious is that blame for the massive spike in many chronic “diseases of civilization” should go to the same cartel. It involves Big Government, Big Food, Big Pharma, Big Media that rely on pharmaceutical industry ad dollars, and medical lobbying outfits such as the American Academy of Pediatrics pretending to be sound science crusaders.
In his speech, Kennedy devoted many paragraphs to the “chronic disease epidemic” – including ever higher rates, even among children, of Type II diabetes and obesity, and of Alzheimer’s, which some now refer to as “Type III diabetes.” He spoke of “the insidious corruption at the FDA and the NIH, the HHS and the USDA that has caused the epidemic,” referring to the Food and Drug Administration, the Department of Health and Human Services, and the U.S. Department of Agriculture, along with the NIH.
But he didn’t stop there. He spoke of “an explosion of neurological illnesses that I never saw as a kid,” including:
ADD, ADHD, speech delay, language delay, Tourette’s Syndrome, narcolepsy, ASD, Asperger’s, autism. In the year 2000, the Autism rate was one in 1500. Now, autism rates in kids are one in 36, according to CDC; nationally, nobody’s talking about this.
He also spoke of the massive spikes in the use of antidepressants and anti-anxiety drugs. Of course, first ladies and surgeons general have launched “healthy lifestyle” campaigns, but these always parrot the conventional wisdom of the cartel. In contrast, Kennedy blamed the cartel itself, not a gluttonous public, for the chronic disease crisis. It was this cartel that gave us the war on healthy dietary fats and the ridiculous food pyramid – heavy on unhealthy ultrarefined carbohydrates and light on fat – which helped make Americans far fatter and sicker than we were before.
His speech hit a nerve, especially among parents who recognize this problem but lack a credible and effective way to fight it. They may engage in private acts of defiance – refusing the COVID-19 or Hepatitis B vaccines for their young children, or disregarding USDA warnings about the consumption of animal fat. So far, however, neither political party has taken up this topic. The Left has tended to give the administrative state the benefit of the doubt. The Right has tended to do the same for corporations.
Trump has promised that Kennedy will have a leading role in fighting America’s health crisis. That will mean taking on the cartel. But the devil is in the details. A sustained effort to “make America healthy again,” or MAHA – to complement MAGA – must be free of government interests on the one hand and industry funding and lobbyists on the other.
Maybe that’s impossible, but Kennedy as MAHA czar could mean a serious exploration of the role the cartel has played in the following:
- Restricting medical freedom
- The origin of the COVID-19 virus
- The effects of the pandemic lockdowns
- The lack of safety and effectiveness of mRNA vaccines
- The rise in childhood and adult obesity
- The rise in childhood and adult Type II diabetes
- The rise in Alzheimer’s
- The rise in allergies, food sensitivities, and asthma
- Rising rates of depression and anxiety disorders
- Rising rates of neurological disorders such as autism
- The explosion of cases of childhood gender dysphoria
- The collusion between the World Professional Association of Transgender Health and HHS officials such as transgender activist and Assistant Secretary for Health Rachel Levine
- The political agenda of transnational public health bureaucracies such as the World Health Organization
- The medicalization of the treatment for gender dysphoria with “gender-affirming care” (rather than taking a mental health approach)
- The capitulation of NIH, CDC, FDA, and HHS to gender ideology over sound science
- The lack of value and safety of the ever-growing childhood vaccine schedule
- The medical focus on symptoms rather than underlying causes and cures of diseases
- The artificial restriction of medical and therapeutic credentialing of professionals to control supply and competition
- The decline in average testosterone in males
- The rise in infertility
- The rise in opioid addiction and overdose deaths
- Unethical research sponsored by the NIH
- The incompetence of the USDA in dispensing nutrition advice
- The effect of agricultural subsidies on our health
- Environmentalist dogmas masquerading as health and nutrition advice
If Trump appoints Kennedy as the MAHA czar, it would be akin to his COVID-19 Operation Warp Speed during his first administration but without the industry taint.
Of course, that appointment could come to nothing – except that there is already a coalition forming of millions of parents across, and even orthogonal to, the political spectrum, who – as Kennedy has put it – love their children more than they hate each other. It would take both the political will in Washington and a popular constituency of average Americans to fight the biomedical security state and the cartel that fuels it.
We’re getting a glimpse of this motley resistance in the unlikely unity ticket of Trump and Kennedy and the many strange bedfellows supporting them. If this coalition outlives the 2024 presidential election, it could reorder our political categories and leave to our children and grandchildren a quite different future.

The Red Deer Regional Health Foundation is thrilled to announce the winners of this year’s Red Deer Hospital Lottery prizes – including the Dream Home, a $100,000.00 cash prize, and Mega Bucks 50.
James Smith of Spruce View has won the $100,000.00 cash prize.
Montey Brehaut of Red Deer has won the Mega Bucks 50 jackpot, taking home $301,702.50.
The grand prize Sorento Custom Homes Dream Home, including furnishings by Urban Barn and worth $1,074,472 – has been awarded to Oscar Gunnlaugson of Sylvan Lake.
The winner announcements took place at noon on June 26 , 2025 – and was streamed live on Facebook from Red Deer Regional Hospital Center.
“We’re excited to celebrate this year’s winners and deeply grateful to everyone who supported the lottery,” said Manon Therriault, CEO of the Red Deer Regional Health Foundation. “Funds raised will directly enhance patient care at Red Deer Regional Hospital Centre.”
This year’s lottery proceeds will fund essential new and replacement equipment, ensuring Red Deer Regional Hospital Center can continue to serve the 500,000 people who rely on it. While plans for the hospital expansion move forward, healthcare doesn’t wait. Patients in our community need access
to life-saving technology today, and supporting Red Deer Hospital Lottery has made that possible.
A full list of winners, including electronics prize recipients, will be posted on July 2 at reddeerhospitallottery.ca.
Winners will also receive instructions on how to claim their prizes by mail.
The keys to the Dream Home will be presented at a special ceremony this summer.

From LifeSiteNews
Research found that men who underwent a ‘gender transition’ using hormones have a 51% higher mortality rate than the general population and a ‘threefold’ greater risk of cardiovascular deaths.
A newly published study has found that males’ use of estrogen to present as “female” triples their risk of cardiovascular disease, while also heightening the risk of stroke, blood clots, depression, and cognitive impairment.
The journal Discover Mental Health on June 12 released a variety of findings regarding the negative impacts of estrogen use in males attempting to transition to “female.” One of the most significant was that current estrogen use “was associated with a threefold increased risk of death from cardiovascular events.”
In fact, a study of 966 “female transitioned” males were found to have a mortality rate 51 percent higher than that of the general population. Their main causes of death included cardiovascular disease (21 percent), cancer (32 percent), suicide (7.5 percent), and infection-related disease (five percent).
Estrogen use by males amplified other cardiovascular risks, especially with prolonged use. One meta-analysis found a 30 percent higher rate of stroke among gender-confused men who took estrogen compared with men who did not.
A review also found “strong evidence” that estrogen use by men increases their risk for vein blood clots “over fivefold.”
Estrogen use was also found to have a detrimental cognitive impact on men. For example, so-called “female transitioned” males were found to have lower scores than both their other male counterparts and women in “information-processing speed and episodic memory.”
In addition, elevated symptoms of depression were “associated with increased serum levels of estradiol” for men under the age of 60.
This recent study confirms 2023 study that found that all gender-confused individuals, whether men attempting to present themselves as women or women attempting to present themselves as men, were at significantly increased risk for a range of deadly cardiovascular conditions, including strokes, heart attacks, high blood pressure, and elevated cholesterol levels.
A 2019 study published by the National Institutes of Health (NIH) National Library of Medicine also found:
Cardiovascular disease (CVD) is the leading disease-specific cause of death for [so-called] transgender people undergoing [transgender procedures], with only suicide claiming more lives as the leader of all cause mortality.
However, for [gender-confused males], the risk of death from CVD is 3-fold higher than for all other groups.
Research reported by both the British Heart Association and the American Heart Association that same year arrived at similar findings:
“We already know sex hormones are important to cardiovascular health, and now we have people being exposed to high levels of sex hormones they normally would not have, which could be associated with cardiovascular benefit or risk,” said Dr. Christian Delles, a professor at the Institute of Cardiovascular and Medical Sciences at the University of Glasgow.


What Connor Should Say To Oilers: It’s Not You. It’s Me.

Top 7 Features Every Canadian Home Care Agency Needs in Their Home Care Software

The U.S. Strike in Iran-Insecurity About Global Oil Supply Suddenly Makes Canadian Oil Attractive

Discover hidden paths – Uncover nature’s secrets in Central Alberta
-
 MAiD2 days ago
MAiD2 days agoCanada’s euthanasia regime is not health care, but a death machine for the unwanted
-
 Alberta2 days ago
Alberta2 days agoAlberta’s government is investing $5 million to help launch the world’s first direct air capture centre at Innisfail
-
 Business2 days ago
Business2 days agoOttawa Funded the China Ferry Deal—Then Pretended to Oppose It
-
 armed forces2 days ago
armed forces2 days agoIt’s not enough to just make military commitments—we must also execute them
-
 Business2 days ago
Business2 days agoCarnival Cinemas moving downtown: Owner Bill Ramji buys former Uptown Cinemas from RDP
-
 armed forces2 days ago
armed forces2 days agoMark Carney Thinks He’s Cinderella At The Ball
-
 Business1 day ago
Business1 day agoBehind the latest CPI Numbers: Inflation Slows, But Living Costs Don’t
-
 Business2 days ago
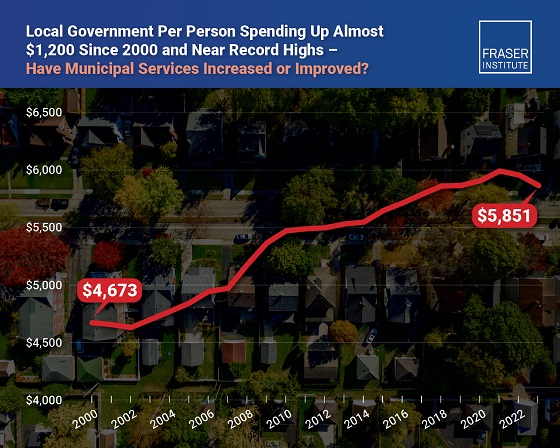
Business2 days agoMunicipal government per-person spending in Canada hit near record levels