COVID-19
Harvard drops COVID vaccine mandate for students; other holdout colleges may follow suit

From LifeSiteNews
Harvard’s reversal constitutes the “beginning of the end of the COVID mandate, the final nail in the coffin.”
Prestigious Harvard University has finally abandoned its COVID-19 vaccine mandate for students, a surrender that could be the first of several dominoes to fall in academia.
Last month, LifeSiteNews reported that medical freedom group No College Mandates had identified 68 of the 1,216 undergraduate institutions of higher learning across the United States as still requiring students to take at least one mRNA COVID shot. The list includes Ivy League Harvard University, which said the shot is required for “all students who will be on campus” and that “registration holds (for classes) will be automatically applied” who “fall(s) out of compliance at any time for any of the required immunizations.” (Students could apply for medical or religious exemptions, however.)
On March 5, however, Harvard University Health Services (HUHS) announced that it “will no longer require students to receive the COVID-19 vaccine.” It continued to “strongly recommend that all members of the Harvard community stay up to date on COVID-19 vaccines, including boosters if eligible,” as well as “high-quality face mask(s) in crowded indoor settings and remaining at home if unwell.”
“This is a big deal. I am literally blown away,” No College Mandates co-founder Lucia Sinatra told The Epoch Times. “For Harvard to remove this language from the immunization forms is a huge sweeping move that is impossible to overstate. As goes Harvard, so goes the rest of the country, and I believe many of the small liberal arts colleges are now going to have a very hard time justifying the demand that young people take these shots now that Harvard has dropped it.”
Sinatra predicted that Harvard’s reversal constitutes the “beginning of the end of the COVID mandate, the final nail in the coffin.”
The COVID vaccines were developed and reviewed in a fraction of the time vaccines usually take under the Trump administration’s Operation Warp Speed initiative. But while initially hailed as an unprecedented achievement embraced by many in both parties, a significant body of evidence has since arisen establishing that they carry significant health risks.
The federal Vaccine Adverse Event Reporting System (VAERS) reports 37,231 deaths, 214,906 hospitalizations, 21,524 heart attacks, and 28,214 myocarditis and pericarditis cases as of February 23, among other ailments. An April 2022 study out of Israel indicates that COVID infection itself cannot fully account for the myocarditis numbers despite common insistence to the contrary. VAERS reports are technically unconfirmed, as anyone can submit one, but U.S. Centers for Disease Control & Prevention (CDC) researchers have recognized a “high verification rate of reports of myocarditis to VAERS after mRNA-based COVID-19 vaccination,” leading to the conclusion that “under-reporting is more likely” than over-reporting.
A 2010 report submitted to the U.S. Department of Health & Human Services’ (HHS’s) Agency for Healthcare Research & Quality (AHRQ) warned that VAERS caught “fewer than 1% of vaccine adverse events.” On the problem of under-reporting, the VAERS website offers only that “more serious and unexpected medical events are probably more likely to be reported than minor ones” (emphasis added).
In 2021, Project Veritas shed light on some of the reasons for such under-reporting with undercover video from inside Phoenix Indian Medical Center, a facility run under HHS’s Indian Health Service program, in which emergency room physician Dr. Maria Gonzales laments that myocarditis cases go unreported “because they want to shove it under the mat,” and nurse Deanna Paris attests to seeing “a lot” of people who “got sick from the side effects” of the COVID shots, but “nobody” is reporting them to VAERS “because it takes over a half hour to write the damn thing.”
Further, VAERS is not the only data source containing red flags. Data from the Pentagon’s Defense Medical Epidemiology Database (DMED) shows that 2021 saw drastic spikes in a variety of diagnoses for serious medical issues over the previous five-year average, including hypertension (2,181%), neurological disorders (1,048%), multiple sclerosis (680%), Guillain-Barre syndrome (551%), breast cancer, (487%), female infertility (472%), pulmonary embolism (468%), migraines (452%), ovarian dysfunction (437%), testicular cancer (369%), and tachycardia (302%).
Last September, the Japanese Society for Vaccinology published a peer-reviewed study conducted by researchers from Stanford, UCLA, and the University of Maryland, which found that the “Pfizer trial exhibited a 36% higher risk of serious adverse events in the vaccine group” while the “Moderna trial exhibited a 6% higher risk of serious adverse events in the vaccine group,” for a combined “16% higher risk of serious adverse events in mRNA vaccine recipients.”
In December 2022, Republican U.S. Sen. Ron Johnson of Wisconsin hosted a roundtable discussion during which civil rights attorney Aaron Siri detailed data from the CDC’s V-Safe reporting system revealing that 800,000 of the system’s 10 million participants, or approximately 7.7%, reported needing medical care after COVID injection. “Twenty-five percent of those people needed emergency care or were hospitalized, and another 48 percent sought urgent care,” Siri added. “Also, another 25 percent on top of the 7.7 percent reported being unable to work or go to school.”
Another study by a team of American, British, and Canadian researchers, published last December in the Journal of Medical Ethics, found that COVID booster mandates for university students – a relatively healthy group at relatively low risk from the virus – do far more harm than good: “per COVID-19 hospitalization prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines, including 1.5-4.6 booster-associated myopericarditis cases in males (typically requiring hospitalization).”
Most recently, an analysis of 99 million people across eight countries published February in the journal Vaccine – the largest analysis to date – “observed significantly higher risks of myocarditis following the first, second and third doses” of mRNA-based COVID vaccines, as well as signs of increased risk of “pericarditis, Guillain-Barré syndrome, and cerebral venous sinus thrombosis,” and other “potential safety signals that require further investigation.”
For those in the academic world still struggling under COVID vaccine mandates, No College Mandates offers on its website a variety of resources to help connect students and staff with resources to find information, counseling, and legal representation.


 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
45.3% of “COVID-19 deaths” in Greece had no symptoms — exposing the coordinated PSYOP deployed to maximize fear and enforce mass compliance with draconian control measures.
The study titled “Deaths “due to” COVID-19 and deaths “with” COVID-19 during the Omicron variant surge, among hospitalized patients in seven tertiary-care hospitals, Athens, Greece” was just published in the journal Scientific Reports:
Abstract
In Greek hospitals, all deaths with a positive SARS-CoV-2 test are counted as COVID-19 deaths. Our aim was to investigate whether COVID-19 was the primary cause of death, a contributing cause of death or not-related to death amongst patients who died in hospitals during the Omicron surge and were registered as COVID-19 deaths. Additionally, we aimed to analyze the factors associated with the classification of these deaths. We retrospectively re-viewed all in-hospital deaths, that were reported as COVID-19 deaths, in 7 hospitals, serving Athens, Greece, from January 1, 2022, until August 31, 2022. We retrieved clinical and laboratory data from patient records. Each death reported as COVID-19 death was characterized as: (A) death “due to” COVID-19, or (B) death “with” COVID-19. We reviewed 530 in-hospital deaths, classified as COVID-19 deaths (52.4% males; mean age 81.7 ± 11.1 years). We categorized 290 (54.7%) deaths as attributable or related to COVID-19 and in 240 (45.3%) deaths unrelated to COVID-19. In multivariable analysis The two groups differed significantly in age (83.6 ± 9.8 vs. 79.9 ± 11.8, p = 0.016), immunosuppression history (11% vs. 18.8%, p = 0.027), history of liver disease (1.4% vs. 8.4%, p = 0.047) and the presence of COVID-19 symptoms (p < 0.001). Hospital stay was greater in persons dying from non-COVID-19 related causes. Among 530 in-hospital deaths, registered as COVID-19 deaths, in seven hospitals in Athens during the Omicron wave, 240 (45.28%) were reassessed as not directly attributable to COVID-19. Accuracy in defining the cause of death during the COVID-19 pandemic is of paramount importance for surveillance and intervention purposes.
 |
Key Findings:
Massive Overcounting of COVID-19 Deaths
- Out of 530 hospital deaths registered as COVID-19 deaths, only 290 (54.7%) were actually caused by COVID-19.
- 240 deaths (45.3%) were found to be completely unrelated to COVID-19 — patients died with a positive PCR test, but showed no symptoms, required no COVID-specific treatment, and died of clearly unrelated causes.
Death Certificate Inaccuracy
- Of the 204 certificates listing COVID-19 as the direct cause of death, only 132 (64.7%) were confirmed as such after clinical review.
- Of the 324 certificates listing COVID-19 as a contributing factor, only 86 (26.5%) were found to be truly related.
Hospital-Acquired Infections Misclassified
- Patients infected during hospitalization were significantly more likely to be misclassified as COVID-19 deaths (OR: 2.3, p = 0.001).
Younger Age and Severe Comorbidities Associated with Misclassification
- Patients who died “with” COVID-19 were younger, more likely to be immunosuppressed, have end-stage liver disease, or be admitted for other causes.
Symptoms and Treatments Differed Sharply
Patients who died “due to” COVID-19 were more likely to:
- Exhibit classic symptoms: hypoxia (44.1%), shortness of breath, fever, and cough
- Require oxygen support (93.4% vs. 66.9%) and receive COVID-specific therapies:
- Remdesivir (5-day course: 61.9% vs. 35.2%)
- Dexamethasone (81.7% vs. 40.7%)
Study Strengths
This study went far beyond death certificate coding, implementing a rigorous, multi-source clinical audit:
- Full medical chart reviews: Included physician notes, lab data, imaging, and treatment records.
- Attending physician interviews: Structured questionnaires captured real-time clinical insights from those who treated the patients.
- Dual independent expert assessments: Two experienced infectious disease specialists (each with >2,500 COVID cases) reviewed each case independently for classification accuracy.
This study found that nearly half of all registered COVID-19 deaths during the Omicron wave in Greece were misclassified, with no clinical evidence linking them to COVID-19 as the true cause. Given that similar death coding practices were employed across Western nations, it is reasonable to conclude that COVID-19 death counts were artificially inflated to a comparable degree elsewhere.
This drastic inflation of death counts aligns with what many now understand to be a coordinated psychological operation (PSYOP)—designed to instill fear and maximize compliance with draconian pandemic measures such as lockdowns, mask mandates, and mass mRNA injection campaigns.
It is this weaponization of fear that has prompted criminal referrals in seven U.S. states, triggering active criminal investigations into top COVID-19 officials for terrorism, murder and racketeering:
BREAKING – The Pandemic Justice Phase Begins as Criminal Investigations Commence |
||||||
|
||||||
 |
||||||
|
By Nicolas Hulscher, MPH
|
||||||
|
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.
2025 Federal Election
Conservatives promise to ban firing of Canadian federal workers based on COVID jab status

From LifeSiteNews
The Conservative platform also vows that the party will oppose mandatory digital ID systems and a central bank digital currency if elected.
Pierre Poilievre’s Conservative Party’s 2025 election platform includes a promise to “ban” the firing of any federal worker based “solely” on whether or not they chose to get the COVID shots.
On page 23 of the “Canada First – For A Change” plan, which was released on Tuesday, the promise to protect un-jabbed federal workers is mentioned under “Protect Personal Autonomy, Privacy, and Data Security.”
It promises that a Conservative government will “Ban the dismissal of federal workers based solely on COVID vaccine status.”
The Conservative Party also promises to “Oppose any move toward mandatory digital ID systems” as well as “Prohibit the Bank of Canada from developing or implementing a central bank digital currency.”
In October 2021, the Liberal government of former Prime Minister Justin Trudeau announced unprecedented COVID-19 jab mandates for all federal workers and those in the transportation sector. The government also announced that the unjabbed would no longer be able to travel by air, boat, or train, both domestically and internationally.
This policy resulted in thousands losing their jobs or being placed on leave for non-compliance. It also trapped “unvaccinated” Canadians in the country.
COVID jab mandates, which also came from provincial governments with the support of the federal government, split Canadian society. The shots have been linked to a multitude of negative and often severe side effects, such as death, including in children.
Many recent rulings have gone in favor of those who chose not to get the shots and were fired as a result, such as an arbitrator ruling that one of the nation’s leading hospitals in Ontario must compensate 82 healthcare workers terminated after refusing to get the jabs.
Beyond health concerns, many Canadians, especially Catholics, opposed the injections on moral grounds because of their link to fetal cell lines derived from the tissue of aborted babies.


The Federal Brief That Should Sink Carney
How Canada’s Mainstream Media Lost the Public Trust

Ottawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
Climate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
2025 Federal Election9 hours ago
The Federal Brief That Should Sink Carney
-
2025 Federal Election11 hours ago
How Canada’s Mainstream Media Lost the Public Trust
-
2025 Federal Election14 hours ago
Ottawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
 2025 Federal Election13 hours ago
2025 Federal Election13 hours agoReal Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
John Stossel10 hours ago
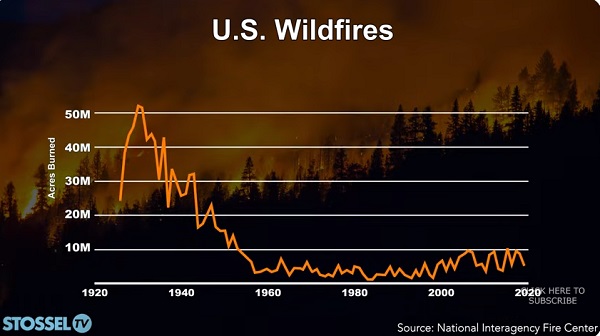
Climate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
COVID-1912 hours ago
Nearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal
-
 Entertainment2 days ago
Entertainment2 days agoPedro Pascal launches attack on J.K. Rowling over biological sex views
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoPoilievre Campaigning To Build A Canadian Economic Fortress