Addictions
When pleasure becomes pain: How substance use damages the body and brain


By Alexandra Keeler
Sustained drug use profoundly impacts brain function and physical health, leading to irreversible damage and long-term health risks
On Jan. 3, the US’s top doctor made headlines for recommending that alcoholic drinks include health warnings about their cancer risks. Alcohol consumption is a leading preventable cause of cancer, U.S. Surgeon General Dr. Vivek Murthy’s advisory notes.
Murthy’s recommendation comes amidst mounting attention to the health risks of alcohol consumption. In 2023, the World Health Organization sparked controversy when it said “no level of alcohol consumption is safe for our health.”
But all substance use affects the body, sources say, with illegal substances damaging nearly every organ in the body. Yet, the health effects of illegal substances receive relatively little attention.
“If you’ve ever looked at a population of people with substance use disorder [and] compared them to the general population, they would be worse off in terms of their cardiovascular risk,” said Dr. Christopher Labos, a Montreal-based cardiologist and host of The Body of Evidence podcast.
Several confounders
Illicit drugs like fentanyl, heroin and cocaine affect the body in all sorts of ways. But isolating their direct effects can be difficult, experts say, due to the social factors that often accompany addiction.
“People who are suffering from substance use disorder probably have poor nutrition, probably don’t exercise as much,” said Labos.
“Anybody who’s suffering from these problems is going to have several confounders that are going to increase the risk of cardiovascular disease.”
But Labos says cocaine is known to be the most damaging to the heart.
“In terms of which [illegal] substances are directly damaging to the heart, we clearly have a number one winner, and that would be cocaine,” Labos said.
“Cocaine is the one that’s very deliberately going to lead to higher rates of atherosclerosis [thickened artery walls] by increasing your heart rate, increasing your blood pressure and actually having a direct effect on thrombosis, so clogging of the arteries,” he added.
Opioids such as fentanyl and heroin also influence heart activity, Labos says. They lengthen the QT interval — a measure of heart electrical activity — which increases the risk of abnormal heart rhythms and potentially life-threatening cardiac issues.
Brain injury is another significant risk associated with illicit drug use.
Mauricio Garcia-Barrera, a psychology professor at the University of Victoria, says opioids such as fentanyl and heroin cause respiratory depression, leading to oxygen deprivation in the brain that damages brain cells.
“Between one to two minutes [after overdose, before resuscitation], the brain damage can start initiating, and between five minutes of cells in the brain not receiving oxygen, then we have the death of brain cells,” said Garcia-Barrera.
By contrast, stimulants like cocaine accelerate brain aging by damaging neurotransmitters, causing grey matter loss that leads to cognitive decline and impaired decision-making.
Our content is always free.
Subscribe to get BTN’s latest news and analysis, or donate to our journalism fund.
Brain changes
Neuropsychologist Carolyn Lemsky is the clinical director of Community Head Injury Resource Services, a Toronto not-for-profit that runs a brain rehabilitation program.
Lemsky says many of her patients want to quit using substances. But habitual drug use alters brain structure and function, making it difficult to quit.
“In people who use opioids and who have a lot of these non-fatal overdoses, their brain changes in many ways,” said Lemsky.
The brain atrophies in critical areas like the hippocampus, the region responsible for memory, and the temporal lobes. Simultaneously, neural pathways linked to habitual behaviour “get a little fatter,” reinforcing addiction.
This rewiring “tilts the brain toward immediate gratification,” Lemsky said. Meanwhile, impairments in the hippocampus diminish the ability to recall the negative consequences of past actions, making recovery even more challenging.
But Lemsky says alcohol remains the most problematic substance for her clients, due to its widespread use.
And while it is a legal substance, alcohol also affects the brain, she says. It leads to cognitive issues like memory and executive functioning problems. Many of her clients develop alcohol-related dementia due to vitamin deficiencies caused by chronic alcohol use.
Cannabis, another legal substance, has also become “more and more problematic” for her clients over the past 15 years, Lemsky says.
“Cannabis also interferes with cognitive functioning,” she said.
According to Health Canada’s 2024 cannabis survey, 80 per cent of Canadians recognize cannabis can be habit-forming and detrimental to youth brain development. Only 71 per cent said they were aware it is linked to mental health issues such as psychosis.
‘Further research is needed’
In a statement to Canadian Affairs, Health Canada said the long-term health consequences of illegal drug use require further study.
“Further research is needed to better understand long-term impacts of opioid-related harms, including the relationship between brain injury and substance use, as well as predisposing factors and long-term effects,” said Marie-Pier Burelle, a media relations advisor for Health Canada.
Lemsky says it is problematic that the Canadian Drugs and Substances Strategy — the government’s framework for addressing substance use-related harms — does not address the known health effects of illegal drugs.
“If you look at the Canada drug strategy, it doesn’t mention brain or cognition once,” she said.
In 2022, NDP MP Alistair MacGregor introduced Bill C-277, a private member’s bill that aims to establish a national strategy on brain injuries. The bill was at the report stage when Parliament was prorogued in early January. Further work on the bill could resume in the next parliamentary session.
“They need a brain injury strategy,” says Lemsky, explaining that cognitive impairment is the leading reason people disengage from medical support services, such as getting treatment for addiction.
“The treatment has too high a cognitive load and isn’t adapted to their needs,” she said. “They can’t manage, and they leave.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Our content is always free.
Subscribe to get BTN’s latest news and analysis, or donate to our journalism fund.
News release from Alberta RCMP
Virtual Opioid Dependency Program serves vulnerable population in Red Deer
Since April 2024, your Alberta RCMP’s Community Safety and Well-being Branch (CSWB) has been piloting the Virtual Opioid Dependency Program (VODP) program in Red Deer to assist those facing opioid dependency with initial-stage intervention services. VODP is a collaboration with the Government of Alberta, Recovery Alberta, and the Alberta RCMP, and was created to help address opioid addiction across the province.
Red Deer’s VODP consists of two teams, each consisting of a police officer and a paramedic. These teams cover the communities of Red Deer, Innisfail, Blackfalds and Sylvan Lake. The goal of the program is to have frontline points of contact that can assist opioid users by getting them access to treatment, counselling, and life-saving medication.
The Alberta RCMP’s role in VODP:
- Conducting outreach in the community, on foot, by vehicle, and even UTV, and interacting with vulnerable persons and talking with them about treatment options and making VODP referrals.
- Attending calls for service in which opioid use may be a factor, such as drug poisonings, open drug use in public, social diversion calls, etc.
- Administering medication such as Suboxone and Sublocade to opioid users who are arrested and lodged in RCMP cells and voluntarily wish to participate in VODP; these medications help with withdrawal symptoms and are the primary method for treating opioid addiction. Individuals may be provided ongoing treatment while in police custody or incarceration.
- Collaborating with agencies in the treatment and addiction space to work together on client care. Red Deer’s VODP chairs a quarterly Vulnerable Populations Working Group meeting consisting of a number of local stakeholders who come together to address both client and community needs.
While accountability for criminal actions is necessary, the Alberta RCMP recognizes that opioid addiction is part of larger social and health issues that require long-term supports. Often people facing addictions are among offenders who land in a cycle of criminality. As first responders, our officers are frequently in contact with these individuals. We are ideally placed to help connect those individuals with the VODP. The Alberta RCMP helps those individuals who wish to participate in the VODP by ensuring that they have access to necessary resources and receive the medical care they need, even while they are in police custody.
Since its start, the Red Deer program has made nearly 2,500 referrals and touchpoints with individuals, discussing VODP participation and treatment options. Some successes of the program include:
- In October 2024, Red Deer VODP assessed a 35-year-old male who was arrested and in police custody. The individual was put in contact with medical care and was prescribed and administered Suboxone. The team members did not have any contact with the male again until April 2025 when the individual visited the detachment to thank the team for treating him with care and dignity while in cells, and for getting him access to treatment. The individual stated he had been sober since, saying the treatment saved his life.
- In May 2025, the VODP team worked with a 14-year-old female who was arrested on warrants and lodged in RCMP cells. She had run away from home and was located downtown using opioids. The team spoke to the girl about treatment, was referred to VODP, and was administered Sublocade to treat her addiction. During follow-up, the team received positive feedback from both the family and the attending care providers.
The VODP provides same-day medication starts, opioid treatment transition services, and ongoing opioid dependency care to people anywhere in Alberta who are living with opioid addiction. Visit vodp.ca to learn more.
“This collaboration between Alberta’s Government, Recovery Alberta and the RCMP is a powerful example of how partnerships between health and public safety can change lives. The Virtual Opioid Dependency Program can be the first step in a person’s journey to recovery,” says Alberta’s Minister of Mental Health and Addiction Rick Wilson. “By connecting people to treatment when and where they need it most, we are helping build more paths to recovery and to a healthier Alberta.”
“Part of the Alberta RCMP’s CSWB mandate is the enhancement of public safety through community partnerships,” says Supt. Holly Glassford, Detachment Commander of Red Deer RCMP. “Through VODP, we are committed to building upon community partnerships with social and health agencies, so that we can increase accessibility to supports in our city and reduce crime in Red Deer. Together we are creating a stronger, safer Alberta.”

By Alexandra Keeler
Across Canada, mobile health models are increasingly being used to offer care to rural and underserved communities
Saskatchewan has launched a small fleet of mobile wellness buses to improve access to primary health care, mental health and addiction services in the province.
The first bus began operating in Regina on Feb. 12. Another followed in Prince Albert on March 21. Saskatoon’s bus was unveiled publicly on April 9. All three are former coach buses that have been retrofitted to provide health care to communities facing barriers to access.
“Mobile health units are proven to improve outcomes for people facing barriers to healthcare,” Kayla DeMong, the executive director of addiction treatment centre Prairie Harm Reduction, told Canadian Affairs in an email.
“We fully support this innovative approach and are excited to work alongside the health bus teams to ensure the people we support receive the care they need, when and where they need it.”
Wellness buses
Like all provinces, Saskatchewan has been grappling with the opioid crisis.
In 2023, an estimated 457 individuals died from overdoses in the province. In 2024, that number fell to 346. But the province continues to struggle with fatal and non-fatal overdoses.
In late February, Saskatoon firefighters responded to more than 25 overdoses in a single 24-hour period. Just over a week later, they responded to 37 overdoses within another 24-hour window.
Saskatchewan’s wellness buses are part of the province’s plan to address these problems. In April 2025, the province announced $2.4 million to purchase and retrofit three coach buses, plus $1.5 million in annual operating funds.
The buses operate on fixed schedules at designated locations around each city. Each bus is staffed with a nurse practitioner, nurse and assessor coordinator who offer services such as overdose reversal kits, addiction medicine and mental health referrals.
“By bringing services directly to where people are, the health buses foster safer, more welcoming spaces and help build trusting relationships between community members and care providers,” said DeMong, executive director of Prairie Harm Reduction.
Saskatoon-based Prairie Harm Reduction is one of the local organizations that partners with the buses to provide additional support services. Prairie Harm Reduction provides a range of family, youth and community supports, and also houses the province’s only fixed supervised consumption site.
The mobile model
Saskatchewan is not the only province using wellness buses. Across Canada, mobile health models are increasingly being used to expand access to care in rural and underserved communities.
In Kingston, Ont., the Street Health Centre operates a retrofitted RV called PORCH (Portable Outreach Care Hub) that serves individuals struggling with homelessness and addiction.
“Our outreach services are extremely popular with our clients and community partners,” Donna Glasspoole, manager at Street Health Centre, said in an emailed statement.
“PORCH hits the road two to three days/week and offers a variety of services, which are dependent on the health care providers and community partners aboard.”
Street Health Centre also has a shuttle service that picks up clients in shelters and brings them to medical clinics or addiction medicine clinics.
The PORCH vehicles are not supported by provincial funding, but instead rely on support from the United Way and other grants. Glasspoole says the centre’s permanent location — which does receive government funding — is more cost-effective to operate.
“The vehicles are expensive to operate and our RV is not great in winter months and requires indoor parking,” she said.

Politically palatable
Many mobile health models currently do not provide controversial services such as supervised drug consumption.
The Saskatchewan Health Authority told Canadian Affairs the province’s new wellness buses will not offer supervised consumption services or safer supply, where drug users are given prescribed opioids as an alternative to toxic street drugs.
“There are no plans to provide supervised consumption services from the wellness buses,” Saskatchewan Health Authority spokesperson Courtney Markewich told Canadian Affairs in a phone call.
This limited scope may make mobile services more politically palatable in provinces that have resisted harm reduction measures.
In Ontario, some harm reduction programs have shifted to mobile models following Premier Doug Ford’s decision to suspend supervised consumption services located within 200 metres of schools and daycares.
In April, Toronto Public Health ended operations at its Victoria Street fixed consumption site, replacing it with street outreach and mobile vans.
The Ontario government’s decision to close the sites is part of a broader pivot away from harm reduction. The province is investing $378 million to transition suspended sites into 19 new “HART Hubs” that offer primary care, mental health, addictions treatment and other supports.
Glasspoole says that what matters most is not whether services are provided at fixed or mobile locations, but how care is delivered.
Models that “reduce barriers to care, [are] non-judgemental, and [are staffed by] trauma-informed providers” are what lead more people toward treatment and recovery, she said in her email.
In Saskatchewan, DeMong hopes the province’s new wellness buses help address persistent service gaps and build trust with underserved communities.
“This initiative is a vital step toward filling long-standing gaps in the continuum of care by providing low-barrier, community-based access to health-care services,” she said.
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle
Power Struggle: Electric vehicles and reality

China undermining American energy independence, report says

Electric vehicle sales are falling hard in BC, and it is time to recognize reality.

Elon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party

Canada Caves: Carney ditches digital services tax after criticism from Trump
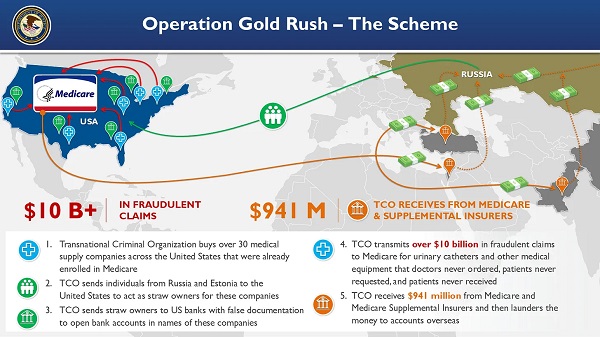
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
Trump on Canada tariff deadline: ‘We can do whatever we want’
-
 Agriculture2 days ago
Agriculture2 days agoCanada’s supply management system is failing consumers
-
 Business1 day ago
Business1 day agoCanada’s loyalty to globalism is bleeding our economy dry
-
 armed forces24 hours ago
armed forces24 hours agoCanada’s Military Can’t Be Fixed With Cash Alone
-
 Alberta1 day ago
Alberta1 day agoCOVID mandates protester in Canada released on bail after over 2 years in jail
-
 Business1 day ago
Business1 day agoCarney’s spending makes Trudeau look like a cheapskate
-
 Alberta23 hours ago
Alberta23 hours agoAlberta Next: Alberta Pension Plan
-
 International1 day ago
International1 day agoTrump transportation secretary tells governors to remove ‘rainbow crosswalks’
-
 Crime1 day ago
Crime1 day agoProject Sleeping Giant: Inside the Chinese Mercantile Machine Linking Beijing’s Underground Banks and the Sinaloa Cartel