Health
Quitting Coffee: Roasting the coffee bean out of my life



Roasting the coffee bean out of my life.
It was a regular morning when I overreacted. Now usually I’m calm, composed, I’m the guy that lets things slide off my shoulder. But on this day, I became a linguist of profanity. It’s not someone I feel I am in my core or someone I consciously strive to be.

I was triggered, triggered by the way my body reacted to the caffeine; it was time to give up coffee.
As a business owner, I get clients that request meetings with me all the time, and who’s business is dependant on the melding of minds, I’m always meeting clients for the first time at trendy coffee shops. So kicking the coffee cup was a conscious decision. Something of which I thought of for a while, but my lack of focus prevented me from achieving the perk-free focus I wanted.
Now, I love coffee, and I have since my mid-twenties since I purchased an espresso machine, which I used for a few months before stuffing it in my cabinet. You see, it wasn’t just the coffee I loved or the caffeine I craved, but I loved the coffee shop culture. It was hip, cool, filled with busy, successful-looking people.
With every order, my inner voice always questioning, “hmm, I wonder what all these $6.50 coffees are doing to my body, should I worry?” or another question I’d ask myself, “am I an addict? Nah,” I’d shrug inside, as I placed an order for a drip coffee with room.
I convinced myself I had my coffee intake under control because I only consumed it around my business meetings, which were, on average, up to 3 times a day. And the caffeine karma was always clean because I would offer to pick up the bill for clients I would meet. “no-no, it’s ok. I got this!” It was full of warm goodness, positive energy over discussions of our software project together, or next movie production, and ideas seemed to explode.
Things changed. It started to become a problem because my want for coffee was percolating between meetings. A promise I made to myself that I’d only consume coffee during meetings, I figured, if I were going to have a bad habit, it would be while I’m going to be productive.
My days started with a morning coffee with my wife during breakfast, then I’d grab a quick cup to sip while coding a software project, or filming, which I’d have close to me on set in a to-go cup, and times it was at night when visiting with friends or family.
It’s only been three days since I’ve quit, it’s been the three most productive days of my life. That’s why I’ve chosen to write this article. I love to write, but while in my coffee-addicted anxious haze, I always had that false sense that I never had the time. But since I’ve quit the bean, I’ve felt present, focused, and just…happy. And now that I’m #CaffeineSober, I realized what coffee and the caffeine in it did to me. I’m sharing this because, a quick google search, I couldn’t find a decent article I could connect with, so I thought I’d write one.
I’m well aware the drug affects people in different ways, but my coffee consumption made me:
- foggy in my mind
- feel like I never had enough time
- react or overreact to stressful events
- feel like I was carrying the weight of the world’s projects
- feel distant from my wife and kids
- feel like I couldn’t handle my daily stress loads and would push myself to get through them.
- not find the joy in the admin tasks of my business, like invoicing, or writing an article like this.
- not want to go to the gym because I would see a workout as an unachievable entire body, two-hour commitment, where now I see them as more focused, micro workouts.
- feel bloated around my waistline
The list goes on, but I didn’t feel GOOD.
I enjoy my coffee with lots of cream and lots of honey. I suspect there’s a possible combination of the three, caffeine, dairy, and sugar, a triple whammy of things which are affecting my mental health, and something I’m going to be tracking, but that’s an entirely different article. But for now, I’m enjoying a flatter stomach as well.
I’m not basing my article off any science. But there seems to be a common observation of the side effects of coffee. According to WebMD, coffee containing caffeine can cause insomnia, nervousness, and restlessness, stomach upset, nausea and vomiting, increased heart and breathing rate, and other side effects.
And if you hold a celebrity’s opinion as an expert’s, here’s an article. Harry Quits Alcohol, Tea, and Coffee for New Year as Meghan’s Healthy Lifestyle Rubs Off
I’m not arguing about the benefits either. I’m sharing my own experience in hopes that if you’re like me, there’s nothing wrong with finding the solution for your happiness.
Roasting the bean from my life hasn’t taken the joy out of meeting clients at trendy coffee shops — sipping something over discussions about video game development, software development, and movie production projects. I’ve switched to teas, I still pick up the bill, and my days are a bit brighter, and my resting-smile-face just a bit larger.
Tell me how quitting coffee has made you feel?
Raoul Bhatt
https://www.facebook.com/BhattTech/
About me, the Author:
I began my career as a graphic artist when I was still in high school, then followed with eight years of developing software before having the courage to create my own Windows XP based software in the mid 2005s with the goal of licensing it to users around the world. During that time, I had a secret passion for film, and making shortfilms and music videos, of which I wasn’t public about…. Fast forward to 2019. I’ve accumulated nearly a million users of my softwares, and developed over 2000 unique projects of which I’ve spent as the writer for, leading and developing my skills for the larger projects I create today which I post frequently on my channels.

From the Fraser Institute
On Monday, the Smith government announced that beginning next year it will change the way it funds surgeries in Alberta. This is a big step towards unlocking the ability of Alberta’s health-care system to provide more, better and faster services for the same or possibly fewer dollars.
To understand the significance of this change, you must understand the consequences of the current (and outdated) approach.
Currently, the Alberta government pays a lump sum of money to hospitals each year. Consequently, hospitals perceive patients as a drain on their budgets. From the hospital’s perspective, there’s little financial incentive to serve more patients, operate more efficiently and provide superior quality services.
Consider what would happen if your local grocery store received a giant bag of money each year to feed people. The number of items would quickly decline to whatever was most convenient for the store to provide. (Have a favourite cereal? Too bad.) Store hours would become less convenient for customers, alongside a general decline in overall service. This type of grocery store, like an Alberta hospital, is actually financially better off (that is, it saves money) if you go elsewhere.
The Smith government plans to flip this entire system on its head, to the benefit of patients and taxpayers. Instead of handing out bags of money each year to providers, the new system—known as “activity-based funding”—will pay health-care providers for each patient they treat, based on the patient’s particular condition and important factors that may add complexity or cost to their care.
This turns patients from a drain on budgets into a source of additional revenue. The result, as has been demonstrated in other universal health-care systems worldwide, is more services delivered using existing health-care infrastructure, lower wait times, improved quality of care, improved access to medical technologies, and less waste.
In other words, Albertans will receive far better value from their health-care system, which is currently among the most expensive in the world. And relief can’t come soon enough—for example, last year in Alberta the median wait time for orthopedic surgeries including hip and knee replacements was 66.8 weeks.
The naysayers argue this approach will undermine the province’s universal system and hurt patients. But by allowing a spectrum of providers to compete for the delivery of quality care, Alberta will follow the lead of other more successful universal health-care systems in countries such as Australia, Germany, the Netherlands and Switzerland and create greater accountability for hospitals and other health-care providers. Taxpayers will get a much better picture of what they’re paying for and how much they pay.
Again, Alberta is not exploring an untested policy. Almost every other developed country with universal health care uses some form of “activity-based funding” for hospital and surgical care. And remember, we already spend more on health care than our counterparts in nearly all of these countries yet endure longer wait times and poorer access to services generally, in part because of how we pay for surgical care.
While the devil is always in the details, and while it’s still possible for the Alberta government to get this wrong, Monday’s announcement is a big step in the right direction. A funding model that puts patients first will get Albertans more of the high-quality health care they already pay for in a timelier fashion. And provide to other provinces an example of bold health-care reform.

Nadeem Esmail
Senior Fellow, Fraser Institute

 From the Montreal Economic Institute
From the Montreal Economic Institute
Alberta’s move to fund acute care services through activity-based funding follows best practices internationally, points out an MEI researcher following an announcement made by Premier Danielle Smith earlier today.
“For too long, the way hospitals were funded in Alberta incentivized treating fewer patients, contributing to our long wait times,” explains Krystle Wittevrongel, director of research at the MEI. “International experience has shown that, with the proper funding models in place, health systems become more efficient to the benefit of patients.”
Currently, Alberta’s hospitals are financed under a system called “global budgeting.” This involves allocating a pre-set amount of funding to pay for a specific number of services based on previous years’ budgets.
Under the government’s newly proposed funding system, hospitals receive a fixed payment for each treatment delivered.
An Economic Note published by the MEI last year showed that Quebec’s gradual adoption of activity-based funding led to higher productivity and lower costs in the province’s health system.
Notably, the province observed that the per-procedure cost of MRIs fell by four per cent as the number of procedures performed increased by 22 per cent.
In the radiology and oncology sector, it observed productivity increases of 26 per cent while procedure costs decreased by seven per cent.
“Being able to perform more surgeries, at lower costs, and within shorter timelines is exactly what Alberta’s patients need, and Premier Smith understands that,” continued Mrs. Wittevrongel. “Today’s announcement is a good first step, and we look forward to seeing a successful roll-out once appropriate funding levels per procedure are set.”
The governments expects to roll-out this new funding model for select procedures starting in 2026.
* * *
The MEI is an independent public policy think tank with offices in Montreal, Ottawa, and Calgary. Through its publications, media appearances, and advisory services to policymakers, the MEI stimulates public policy debate and reforms based on sound economics and entrepreneurship.


Poilievre To Create ‘Canada First’ National Energy Corridor

Trump Takes More Action To Get Government Out Of LNG’s Way

Mainstream Media Election Coverage: If the Election Was a NHL Game, the Ice Would be Constantly Tilted Up and to the Left

Selective reporting on measles outbreaks is a globalist smear campaign against Trump administration.

Highly touted policies the Liberal government didn’t actually implement

Will Four More Years Of Liberals Prove The West’s Tipping Point?

Auto giant shuts down foreign plants as Trump moves to protect U.S. industry
-
 Bruce Dowbiggin2 days ago
Bruce Dowbiggin2 days agoBettman Gives Rogers Keys To The Empire. Nothing Will Change
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoPoilievre Will Bring in ‘One and Done’ Resource Approvals, and Ten Specific Projects Including LNG Canada Phase II
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoElection Security Briefing Confirms CCP-Linked Operation Boosted Carney
-
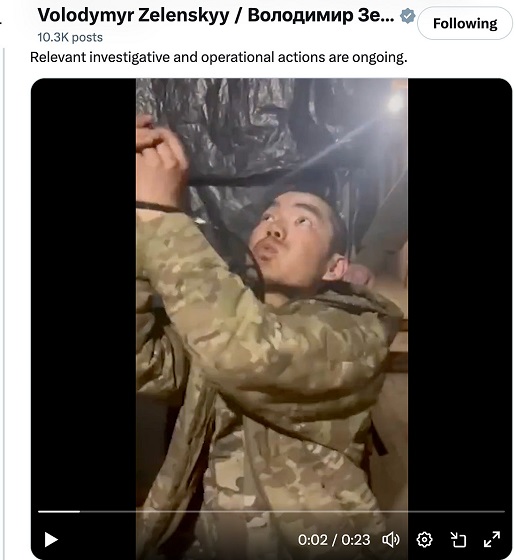 conflict2 days ago
conflict2 days agoZelensky Alleges Chinese Nationals Fighting for Russia, Calls for Global Response
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoHarper Endorses Poilievre at Historic Edmonton Rally: “This Crisis Was Made in Canada”
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoAn In-Depth Campaign Trail “Interview” With Pierre Poilievre
-
Alberta20 hours ago
Alberta’s embrace of activity-based funding is great news for patients
-
 John Stossel20 hours ago
John Stossel20 hours agoGovernment Gambling Hypocrisy: Bad Odds and No Competition
You must be logged in to post a comment Login