COVID-19
Regulatory body continues prosecution of nurse over free expression

From the Justice Centre for Constitutional Freedoms
REGINA, SK: The Justice Centre announces that the disciplinary hearings against Saskatchewan nurse Leah McInnes continue today in what could become a landmark decision about freedom of expression for nurses and other professionals, and the power of regulatory bodies to control and censor the speech of professionals who are required to belong to a professional association in order to earn a living.
Exercising her Charter freedoms of expression, association and peaceful assembly, Saskatchewan Nurse Leah McInnes attended a national rally against mandatory Covid vaccination policies in early September 2021. Ms. McInnes also expressed her opposition to the government’s mandatory vaccination policies on social media between August and October 2021, even while stating that vaccines should be promoted by her profession, that vaccines can decrease severe disease, reduce the burden on the healthcare system and save lives, and that vaccines play a vital role in the fight against the Covid pandemic and should be promoted.
On September 26, 2021, a nurse filed a complaint against Ms. McInnes to the College of Registered Nurses of Saskatchewan (CRNS). The Discipline Committee of the CRNS investigated the social media activities of Ms. McInnes and then charged her with professional misconduct under the Registered Nurses Act for her posts and for her participation in the rally. The CRNS accused Ms. McInnes of spreading misinformation, disinformation and/or misleading information surrounding vaccine mandates and vaccine passports. Further, the Disciplinary Committee of the CRNS alleged that Ms. McInnes had been operating from a position of power as a nurse when participating in the rally and when posting about vaccines, that she had misused this power, and that she had acted outside the proper scope of this power.
Lawyers acting for Ms. McInnes point to the Code of Ethics for Registered Nurses of the CRNS, which says, “Nurses support a climate of trust that sponsors openness, encourages the act of questioning the status quo and supports those who speak out in good faith to address concerns.” Lawyers argue that Ms. McInnes had questioned the merits of mandatory vaccine policies in good faith. Further, counsel for Ms. McInnes argue that her expression, however disagreeable it may have been to the CRNS, is protected by section 2 of the Canadian Charter of Rights and Freedoms and by relevant case law.
In particular, counsel for Ms. McInnes point to the Saskatchewan Court of Appeal ruling in Strom v. Saskatchewan Registered Nurses’ Association, which states that “…criticism, even by those delivering those services, does not necessarily undermine confidence in healthcare workers or the healthcare system. Indeed, it can enhance confidence by demonstrating that those with the greatest knowledge of this massive and opaque system, and who have the ability to affect change, are both prepared and permitted to speak and pursue positive change. In any event, the fact that public confidence in aspects of the healthcare system may suffer as a result of fair criticism can itself result in positive change. Such is the messy business of democracy.”
Lawyers for Ms. McInnes argue that, rather than bringing the nursing profession under disrepute, the good-faith objections to mandatory vaccination policies promote public confidence in the transparency of the healthcare system and in the dedication of healthcare professionals to pursue positive change.
Andre Memauri, one of the lawyers representing Ms. McInnes, stated, “The Discipline Committee today will hear how Ms. McInnes advocated against vaccine mandates and vaccine passports in support of patient autonomy, dignity and privacy in compliance with her ethical obligations. The Investigation Committee alleges Ms. McInnes disseminated misinformation, disinformation and misleading information, all while the record established that Ms. McInnes was not only remarkably accurate but also that the social media activity of CRNS itself disseminated false information.”
“It is very unfortunate that a registered nurse in the Province of Saskatchewan again faces regulatory reprisal for fair criticism of the healthcare system, after the Court of Appeal’s decision in Strom,” continued Mr. Memauri.
John Carpay, President of the Justice Centre, stated, “This case is about the freedom of nurses and other professionals to participate, as citizens in a democracy, in public discussions and debate. This case raises important questions about whether government agencies like the College of Registered Nurses of Saskatchewan should have the power to determine what is true or false, and to impose that determination on professionals who are required to join the regulatory body in order to practice their profession and earn a living.”

 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
As millions of Americans anxiously await action from the new HHS leadership against the COVID-19 mRNA injections—injected into over 9 million children this year—Robert F. Kennedy Jr. has finally gone publicly on the offensive:
Let’s go over each key point made by RFK Jr.:
The recommendation for children was always dubious. It was dubious because kids had almost no risk for COVID-19. Certain kids that had very profound morbidities may have a slight risk. Most kids don’t.
In the largest review to date on myocarditis following SARS-CoV-2 infection vs. COVID-19 vaccination, Mead et al found that vaccine-induced myocarditis is not only significantly more common but also more severe—particularly in children and young males. Our findings make clear that the risks of the shots overwhelmingly outweigh any theoretical benefit:
 |
The OpenSAFELY study included more than 1 million adolescents and children and found that myocarditis was documented ONLY in COVID-19 vaccinated groups and NOT after COVID-19 infection. There were NO COVID-19-related deaths in any group. A&E attendance and unplanned hospitalization were higher after first vaccination compared to unvaccinated groups:
So why are we giving this to tens of millions of kids when the vaccine itself does have profound risk? We’ve seen huge associations of myocarditis and pericarditis with strokes, with other injuries, with neurological injuries.
The two largest COVID-19 vaccine safety studies ever conducted, involving 99 million (Faksova et al) and 85 million people (Raheleh et al), confirm RFK Jr.’s concerns, documenting significantly increased risks of serious adverse events following vaccination, including:
- Myocarditis (+510% after second dose)
- Acute Disseminated Encephalomyelitis (+278% after first dose)
- Cerebral Venous Sinus Thrombosis (+223% after first dose)
- Guillain-Barré Syndrome (+149% after first dose)
- Heart Attack (+286% after second dose)
- Stroke (+240% after first dose)
- Coronary Artery Disease (+244% after second dose)
- Cardiac Arrhythmia (+199% after first dose)
 |
And this was clear even in the clinical data that came out of Pfizer. There were actually more deaths. There were about 23% more deaths in the vaccine group than the placebo group. We need to ask questions and we need to consult with parents.
Actually, according to the Pfizer’s clinical trial data, there were 43% more deaths in the vaccine group compared to the placebo group when post-unblinding deaths are included:
 |
We need to give people informed consent, and we shouldn’t be making recommendations that are not good for the population.
Public acknowledgment of the grave harms of COVID-19 vaccines signals that real action is right around the corner. However, we must hope that action is taken for ALL age groups, as no one is spared from their life-reducing effects:
Alessandria et al (n=290,727, age > 10 years): People vaccinated with 2 doses lost 37% of life expectancy compared to the unvaccinated population during follow-up.
 |
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.


 Nicolas Hulscher, MPH
Nicolas Hulscher, MPH
45.3% of “COVID-19 deaths” in Greece had no symptoms — exposing the coordinated PSYOP deployed to maximize fear and enforce mass compliance with draconian control measures.
The study titled “Deaths “due to” COVID-19 and deaths “with” COVID-19 during the Omicron variant surge, among hospitalized patients in seven tertiary-care hospitals, Athens, Greece” was just published in the journal Scientific Reports:
Abstract
In Greek hospitals, all deaths with a positive SARS-CoV-2 test are counted as COVID-19 deaths. Our aim was to investigate whether COVID-19 was the primary cause of death, a contributing cause of death or not-related to death amongst patients who died in hospitals during the Omicron surge and were registered as COVID-19 deaths. Additionally, we aimed to analyze the factors associated with the classification of these deaths. We retrospectively re-viewed all in-hospital deaths, that were reported as COVID-19 deaths, in 7 hospitals, serving Athens, Greece, from January 1, 2022, until August 31, 2022. We retrieved clinical and laboratory data from patient records. Each death reported as COVID-19 death was characterized as: (A) death “due to” COVID-19, or (B) death “with” COVID-19. We reviewed 530 in-hospital deaths, classified as COVID-19 deaths (52.4% males; mean age 81.7 ± 11.1 years). We categorized 290 (54.7%) deaths as attributable or related to COVID-19 and in 240 (45.3%) deaths unrelated to COVID-19. In multivariable analysis The two groups differed significantly in age (83.6 ± 9.8 vs. 79.9 ± 11.8, p = 0.016), immunosuppression history (11% vs. 18.8%, p = 0.027), history of liver disease (1.4% vs. 8.4%, p = 0.047) and the presence of COVID-19 symptoms (p < 0.001). Hospital stay was greater in persons dying from non-COVID-19 related causes. Among 530 in-hospital deaths, registered as COVID-19 deaths, in seven hospitals in Athens during the Omicron wave, 240 (45.28%) were reassessed as not directly attributable to COVID-19. Accuracy in defining the cause of death during the COVID-19 pandemic is of paramount importance for surveillance and intervention purposes.
 |
Key Findings:
Massive Overcounting of COVID-19 Deaths
- Out of 530 hospital deaths registered as COVID-19 deaths, only 290 (54.7%) were actually caused by COVID-19.
- 240 deaths (45.3%) were found to be completely unrelated to COVID-19 — patients died with a positive PCR test, but showed no symptoms, required no COVID-specific treatment, and died of clearly unrelated causes.
Death Certificate Inaccuracy
- Of the 204 certificates listing COVID-19 as the direct cause of death, only 132 (64.7%) were confirmed as such after clinical review.
- Of the 324 certificates listing COVID-19 as a contributing factor, only 86 (26.5%) were found to be truly related.
Hospital-Acquired Infections Misclassified
- Patients infected during hospitalization were significantly more likely to be misclassified as COVID-19 deaths (OR: 2.3, p = 0.001).
Younger Age and Severe Comorbidities Associated with Misclassification
- Patients who died “with” COVID-19 were younger, more likely to be immunosuppressed, have end-stage liver disease, or be admitted for other causes.
Symptoms and Treatments Differed Sharply
Patients who died “due to” COVID-19 were more likely to:
- Exhibit classic symptoms: hypoxia (44.1%), shortness of breath, fever, and cough
- Require oxygen support (93.4% vs. 66.9%) and receive COVID-specific therapies:
- Remdesivir (5-day course: 61.9% vs. 35.2%)
- Dexamethasone (81.7% vs. 40.7%)
Study Strengths
This study went far beyond death certificate coding, implementing a rigorous, multi-source clinical audit:
- Full medical chart reviews: Included physician notes, lab data, imaging, and treatment records.
- Attending physician interviews: Structured questionnaires captured real-time clinical insights from those who treated the patients.
- Dual independent expert assessments: Two experienced infectious disease specialists (each with >2,500 COVID cases) reviewed each case independently for classification accuracy.
This study found that nearly half of all registered COVID-19 deaths during the Omicron wave in Greece were misclassified, with no clinical evidence linking them to COVID-19 as the true cause. Given that similar death coding practices were employed across Western nations, it is reasonable to conclude that COVID-19 death counts were artificially inflated to a comparable degree elsewhere.
This drastic inflation of death counts aligns with what many now understand to be a coordinated psychological operation (PSYOP)—designed to instill fear and maximize compliance with draconian pandemic measures such as lockdowns, mask mandates, and mass mRNA injection campaigns.
It is this weaponization of fear that has prompted criminal referrals in seven U.S. states, triggering active criminal investigations into top COVID-19 officials for terrorism, murder and racketeering:
BREAKING – The Pandemic Justice Phase Begins as Criminal Investigations Commence |
||||||
|
||||||
 |
||||||
|
By Nicolas Hulscher, MPH
|
||||||
|
Epidemiologist and Foundation Administrator, McCullough Foundation
Please consider following both the McCullough Foundation and my personal account on X (formerly Twitter) for further content.

BREAKING from THE BUREAU: Pro-Beijing Group That Pushed Erin O’Toole’s Exit Warns Chinese Canadians to “Vote Carefully”

Canada drops retaliatory tariffs on automakers, pauses other tariffs

Ex-NYPD Cop Jailed in Beijing’s Transnational Repatriation Plot, Canada Remains Soft Target

The Net-Zero Dream Is Unravelling And The Consequences Are Global

The “Hardhat Vote” Has Embraced Pierre Poilievre

The Pandemic Justice Phase Begins as Criminal Investigations Commence

CPP another example of Albertans’ outsized contribution to Canada
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoOttawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoBREAKING: THE FEDERAL BRIEF THAT SHOULD SINK CARNEY
-
COVID-192 days ago
Nearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoHow Canada’s Mainstream Media Lost the Public Trust
-
 2025 Federal Election19 hours ago
2025 Federal Election19 hours agoMark Carney Wants You to Forget He Clearly Opposes the Development and Export of Canada’s Natural Resources
-
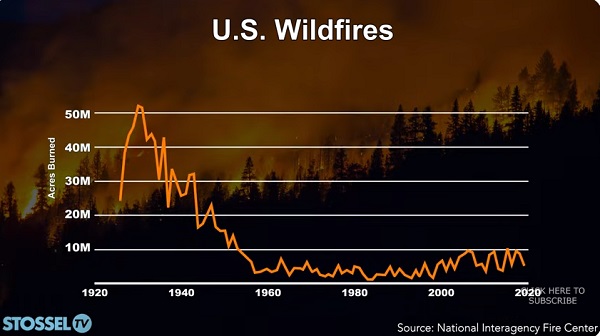 John Stossel2 days ago
John Stossel2 days agoClimate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoCHINESE ELECTION THREAT WARNING: Conservative Candidate Joe Tay Paused Public Campaign
-
 International12 hours ago
International12 hours agoPope Francis’ body on display at the Vatican until Friday