Brownstone Institute
Eye Protection Wasn’t Misdirection

From the Brownstone Institute
“If you have goggles or an eye shield, you should use it.” ~ Anthony Fauci, July 30th, 2020
We had heard enough from Fauci by the time this comment was made in mid-2020 to begin automatically tuning out his frequently contradictory advice. What if we had given weight to this comment and explored why he began recommending goggles (yet never donned them himself)?
While I’m not surprised that the inner anatomy of the face including ocular ducts and connectivity within structures aren’t common knowledge, I expected more of a reaction from the medical community regarding Fauci’s push for eye protection. Not only do medical professionals take extensive coursework on human anatomy — they are required to meet annually with an Industrial Hygienist for fit tested, hazard-specific kit for each exposure setting , including ocular protection. This testing process requires going into detail about each exposure setting and required donning and donning practices within the scope of their professional duties.
Instead of elaborating on his recommendation, Fauci just publicly hushed on the issue and folks carried on, obediently masked up yet entirely neglectful of their nasolacrimal ducts. Shame, shame.

These are the structures of the lacrimal apparatus connecting ocular and nasal pathways. Basically, the eye drains into the nasal cavity. None of the talking heads of the medical community ever seem to bring up that these parts of the body connect with one another, and while we hear about masks ad nauseam three entire years after the onset of the SARS-CoV-2 pandemic, no one is arguing with strangers on the internet about goggles.
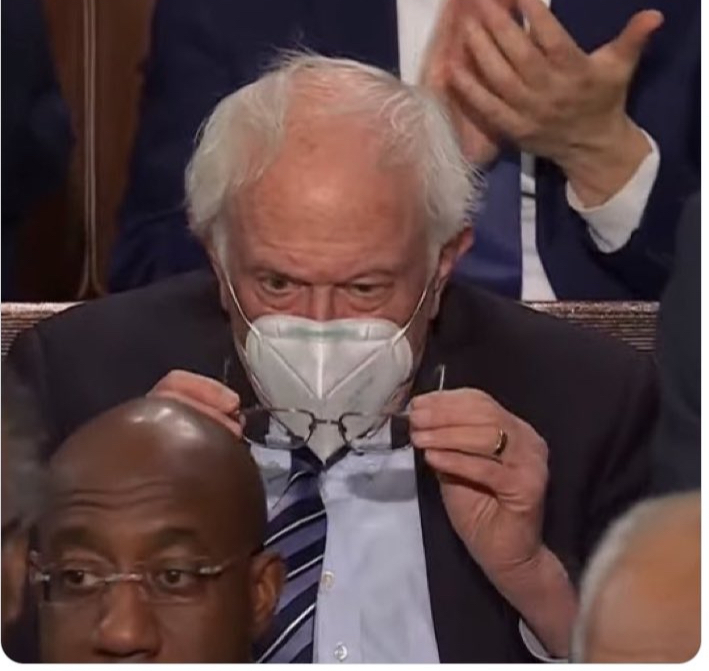
Bernie Sanders was recently praised for being the only person at the February, 2023 State of the Union donning a (sub-grade, non-mitigating) respirator, but eye spy something fishy. It was noted that he kept removing his glasses, as they were fogging up.

Those who have donned respirators have experienced that exhale emissions are generally redirected out of the nose bridge (or out of side gaps if improperly sealed). This is the exhale emission plume create by a fitted, unvalved N95 respirator:

This plume of warm, moist respiratory emissions is what causes glasses to fog. This is precisely why I continue to argue that masks are NOT source control for respiratory aerosols, because these apparatuses are not designed nor intended to protect others from your emissions, but solely for protection of the wearer. The ASTM agrees with me on this matter:
The American Society for Testing and Materials (ASTM) Standard Specification for Barrier Face Coverings F3502-21 Note 2 states, “There are currently no established methods for measuring outward leakage from a barrier face covering, medical mask, or respirator. Nothing in this standard addresses or implies a quantitative assessment of outward leakage and no claims can be made about the degree to which a barrier face covering reduces emission of human-generated particles.”
Additionally, Note 5 states, “There are currently no specific accepted techniques that are available to measure outward leakage from a barrier face covering or other products. Thus, no claims may be made with respect to the degree of source control offered by the barrier face covering based on the leakage assessment.”
So does it matter if your neighbor’s exhale emissions are directed in your face for the duration of your 6-hour flight?

Absolutely. Imagine sitting between these two fine fellas with your eyes exposed, and their emission plumes directed right in your face.
In mitigation of aerosol hazards, eye protection is a standard part of required kit, because those from the correct domain of expertise, Industrial Hygiene, know enough about human anatomy to remember the interconnectivity of facial structures.
Ocular transmission of SARS-CoV-2
There has been a great deal of focus on respiratory protection since the start of the pandemic, but ocular transmission was already established for SARS-CoV-1.
“SARS-CoV-1 has been shown to be transmitted through direct contact or with droplet or aerosolized particle contact with the mucous membranes of the eyes, nose and mouth. Indeed, during the 2003 SARS-CoV-1 outbreak in Toronto, health care workers who failed to wear eye protection in caring for patients infected with SARS-CoV-1 had a higher rate of seroconversion.”
We are beginning to see mounting research on ocular transmission for SARS-CoV-2 emerge, as well, traveling through the nasolacrimal duct from the eye, draining into the sinus cavity.
“There is evidence that SARS-CoV-2 may either directly infect cells on the ocular surface, or virus can be carried by tears through the nasolacrimal duct to infect the nasal or gastrointestinal epithelium.”
“The nasolacrimal system provides an anatomic connection between the ocular surface and the upper respiratory tract. When a drop is instilled into the eye, even though some of it is absorbed by the cornea and the conjunctiva, most of it is drained into the nasal cavity through the nasolacrimal canal and is subsequently transferred to the upper respiratory or the gastrointestinal tract.”
“SARS-CoV-2 on the ocular surface can be transferred to different systems along with tears through the nasolacrimal route.”
Seldom did ocular exposure result in eye infection, while systemic infections occurred regularly. Ocular exposure cannot always be determined as the point of contact for this reason, as an eye infection does not always coincide with systemic infection.
The nasolacrimal duct is often discussed in ocular transmission research, but this is not the sole ocular transmission pathway discussed.
“There are two pathways by which ocular exposure could lead to systemic transmission of the SARS-CoV-2 virus. (1) Direct infection of ocular tissues including cornea, conjunctiva, lacrimal gland, meibomian glands from virus exposure and (2) virus in the tears, which then goes through the nasolacrimal duct to infect the nasal or gastrointestinal epithelium.”
Additionally, research is being conducted on the usage of ocular secretions in transmitting SARS-CoV-2.
“Then here comes the question, whether SARS-CoV-2 detected in conjunctival secretions and tears is an infectious virus? Colavita et al inoculated Vero E6 cells with the first RNA positive ocular sample obtained from a COVID-19 patient. Cytopathic effect was observed 5 days post-inoculation, and viral replication was confirmed by real-time RT-PCR in spent cell medium. Hui et al also isolated SARS-CoV-2 virus from a nasopharyngeal aspirate specimen and a throat swab of a COVID-19 patient. The isolated virus not only infected human conjunctival explants but also infected more extensively and reached higher infectious viral titers than SARS-CoV.”
According to this study, ocular secretions were highly infectious.
“The ocular surface can serve as a reservoir and source of contagion for SARS-CoV-2. SARS-CoV-2 can be transmitted to the ocular surface through hand-eye contact and aerosols, and then transfer to other systems through nasolacrimal route and hematogenous metastasis. The possibility of ocular transmission of SARS-CoV-2 cannot be ignored.”
This paper also has a focus on aerosols coming into contact with ocular mucosa.
“Once aerosols form, SARS-CoV-2 can bind to the ACE2 on the exposed ocular mucosa to cause infection. In order to prevent aerosols from contacting the eye surface, eye protection cannot be ignored.”
An additional area explored in this analysis discusses rhesus macaques wherein solely those inoculated through the ocular route became infected.
“If the ocular surface is the portal for SARS-CoV-2 to enter, where does the virus transfer after entering? An animal experiment reveals the possible nasolacrimal routes of SARS-CoV-2 transfer from the ocular surface. Five rhesus macaques were inoculated with 1×106 50% tissue-culture infectious doses of SARS-CoV-2. Only in the conjunctival swabs of rhesus macaques inoculated via conjunctival route could the SARS-CoV-2 be detected. Conjunctival swabs of the rhesus macaques that were inoculated via intragastric or intratracheal route were negative. Three days post conjunctival inoculation, rhesus macaques presented mild interstitial pneumonia. Autopsies showed that SARS-CoV-2 was detectable in the nasolacrimal system tissues, including the lacrimal gland, conjunctiva, nasal cavity, and throat, which connected the eyes and respiratory tract on anatomy.”
An additional macaque study had similar findings.
“Deng et al. showed that SARS-CoV-2 infection could be induced by ocular surface inoculation in an experimental animal model using macaques. Although the researchers detected the virus in conjunctival swabs only on the first day after inoculation, they continued to detect it in nasal and throat swabs 1-7 days after the inoculation. Their findings demonstrated that the viral load in the airway mucosa was much higher than that in the ocular surface. They euthanized and necropsied one of the conjunctival inoculated-animals and found that the virus had spread to the nasolacrimal system and ocular tissue, nasal cavity, pharynx, trachea, tissues in the oral cavity, tissues in the lower-left lobe of the lung, inguinal and perirectal lymph node, stomach, duode-num, cecum, and ileum. They also found a specific IgG antibody, indicating that the animal was infected with SARS-CoV-2 via the ocular surface route.”
While the nasolacrimal route is the primary focus in most current research, the blood-retinal barrier (BRB) is also discussed as a possible pathway.
“Once it reaches the ocular surface, SARS-CoV-2 could invade the conjunctiva and iris under the mediation of ACE2 and CD147, another possible receptor for SARS-CoV-2 on host cells. De Figueiredo et al described the following possible pathways. After reaching blood capillaries and then choroid plexus, the virus reaches the blood-retinal barrier (BRB), which expresses both ACE2 and CD147 in retinal pigment epithelial cells and blood vessel endothelial cells. Since CD147 mediates the breakdown of neurovascular blood barriers, the virus can cross the BRB and enter into blood.”
RSV
There has been a push recently to bring back masks for Respiratory Syncytial Virus (RSV), especially in schools, as this pathogen largely impacts youth populations, yet ocular transmission is a proven method of infectivity for RSV.
In this paper, intranasal dosing of the given pathogen resulted in onset of illness for nearly all respiratory pathogens studied. It reviews transmission routes and minimum infective dose for Influenza, Rhinovirus, Coxsackievirus, Adenovirus, RSV, Enteric Viruses, Rotavirus, Norovirus, and Echovirus, including ocular transmission.
“The infective doses of rhinoviruses in the nose and eyes are thought to be comparable because the virus does not infect the eyes but appears to travel from the eyes to the nasal mucosa via the tear duct.”
“Hall et al. (1981) investigated the infectivity of RSV A2 strain administered by nose, eye, and mouth in adult volunteers. They reported that the virus may infect by eye or nose and both routes appear to be equally sensitive. A dose of 1.6 × 105 TCID50 infected three of the four volunteers given either into the eyes or nose while only one out of the eight were infected via mouth inoculation, and this was thought to be due to secondary spread of the virus.”
“RSV A2 had poor infectivity when administered via the mouth but was shown to infect by eye and nose and both routes appear to be equally sensitive to the virus.”
“Bynoe et al. (1961) found that colds could be produced almost as readily by applying virus by nasal and conjunctival swabs as by giving nasal drops to volunteers.”
Would masks save schools from RSV circulation? Most kids have robust immune systems, with a very, very small percentage of the youth population undergoing chemotherapy or taking immunosuppressives, who usually are not on campus for in-person learning. But for those seeming protection and in-person instruction, we must not set them up for immune bombardment by offering a false sense of security while feigning ignorance of other viable transmission routes. Masks are not the answer.
Summary
Ocular transmission of respiratory pathogens hasn’t been a focal point of study, but with other pathogens and mounting research on SARS-CoV-2 showing such ease of systemic onset for this transmission route, more attention should be given to this area of research.
Consider all of the people you’ve seen donning masks or respirators over these past three years, assured in the merit of their virtue. How many still got sick? Did you ever once see someone donning goggles? Are we ever going to get around to discussing exhaustion of the hierarchy of controls, or are actual mitigating measures too taboo, too fringe?
TLDR: Ocular transmission is a viable method of transmission for SARS-CoV-2. Masks are not source control. Even N95s aren’t going to fix this. And all child masks are unregulated, untested, unethical, and unsafe, with zero efficacy, fit, term of wear, or medical clearance standards, and with ocular transmission being a proven route of transmission for RSV, masks aren’t going to fix that issue, either.
Author


From the Brownstone Institute
By 
Who Controls the Administrative State?
President Trump on March 20, 2025, ordered the following: “The Secretary of Education shall, to the maximum extent appropriate and permitted by law, take all necessary steps to facilitate the closure of the Department of Education.”
That is interesting language: to “take all necessary steps to facilitate the closure” is not the same as closing it. And what is “permitted by law” is precisely what is in dispute.
It is meant to feel like abolition, and the media reported it as such, but it is not even close. This is not Trump’s fault. The supposed authoritarian has his hands tied in many directions, even over agencies he supposedly controls, the actions of which he must ultimately bear responsibility.
The Department of Education is an executive agency, created by Congress in 1979. Trump wants it gone forever. So do his voters. Can he do that? No but can he destaff the place and scatter its functions? No one knows for sure. Who decides? Presumably the highest court, eventually.
How this is decided – whether the president is actually in charge or really just a symbolic figure like the King of Sweden – affects not just this one destructive agency but hundreds more. Indeed, the fate of the whole of freedom and functioning of constitutional republics may depend on the answer.
All burning questions of politics today turn on who or what is in charge of the administrative state. No one knows the answer and this is for a reason. The main functioning of the modern state falls to a beast that does not exist in the Constitution.
The public mind has never had great love for bureaucracies. Consistent with Max Weber’s worry, they have put society in an impenetrable “iron cage” built of bloodless rationalism, needling edicts, corporatist corruption, and never-ending empire-building checked by neither budgetary restraint nor plebiscite.
Today’s full consciousness of the authority and ubiquity of the administrative state is rather new. The term itself is a mouthful and doesn’t come close to describing the breadth and depth of the problem, including its root systems and retail branches. The new awareness is that neither the people nor their elected representatives are really in charge of the regime under which we live, which betrays the whole political promise of the Enlightenment.
This dawning awareness is probably 100 years late. The machinery of what is popularly known as the “deep state” – I’ve argued there are deep, middle, and shallow layers – has been growing in the US since the inception of the civil service in 1883 and thoroughly entrenched over two world wars and countless crises at home and abroad.
The edifice of compulsion and control is indescribably huge. No one can agree precisely on how many agencies there are or how many people work for them, much less how many institutions and individuals work on contract for them, either directly or indirectly. And that is just the public face; the subterranean branch is far more elusive.
The revolt against them all came with the Covid controls, when everyone was surrounded on all sides by forces outside our purview and about which the politicians knew not much at all. Then those same institutional forces appear to be involved in overturning the rule of a very popular politician whom they tried to stop from gaining a second term.
The combination of this series of outrages – what Jefferson in his Declaration called “a long train of abuses and usurpations, pursuing invariably the same Object” – has led to a torrent of awareness. This has translated into political action.
A distinguishing mark of Trump’s second term has been an optically concerted effort, at least initially, to take control of and then curb administrative state power, more so than any executive in living memory. At every step in these efforts, there has been some barrier, even many on all sides.
There are at least 100 legal challenges making their way through courts. District judges are striking down Trump’s ability to fire workers, redirect funding, curb responsibilities, and otherwise change the way they do business.
Even the signature early achievement of DOGE – the shuttering of USAID – has been stopped by a judge with an attempt to reverse it. A judge has even dared tell the Trump administration who it can and cannot hire at USAID.
Not a day goes by when the New York Times does not manufacture some maudlin defense of the put-upon minions of the tax-funded managerial class. In this worldview, the agencies are always right, whereas any elected or appointed person seeking to rein them in or terminate them is attacking the public interest.
After all, as it turns out, legacy media and the administrative state have worked together for at least a century to cobble together what was conventionally called “the news.” Where would the NYT or the whole legacy media otherwise be?
So ferocious has been the pushback against even the paltry successes and often cosmetic reforms of MAGA/MAHA/DOGE that vigilantes have engaged in terrorism against Teslas and their owners. Not even returning astronauts from being “lost in space” has redeemed Elon Musk from the wrath of the ruling class. Hating him and his companies is the “new thing” for NPCs, on a long list that began with masks, shots, supporting Ukraine, and surgical rights for gender dysphoria.
What is really at stake, more so than any issue in American life (and this applies to states around the world) – far more than any ideological battles over left and right, red and blue, or race and class – is the status, power, and security of the administrative state itself and all its works.
We claim to support democracy yet all the while, empires of command-and-control have arisen among us. The victims have only one mechanism available to fight back: the vote. Can that work? We do not yet know. This question will likely be decided by the highest court.
All of which is awkward. It is impossible to get around this US government organizational chart. All but a handful of agencies live under the category of the executive branch. Article 2, Section 1, says: “The executive Power shall be vested in a President of the United States of America.”

Does the president control the whole of the executive branch in a meaningful way? One would think so. It’s impossible to understand how it could be otherwise. The chief executive is…the chief executive. He is held responsible for what these agencies do – we certainly blasted away at the Trump administration in the first term for everything that happened under his watch. In that case, and if the buck really does stop at the Oval Office desk, the president must have some modicum of control beyond the ability to tag a marionette to get the best parking spot at the agency.
What is the alternative to presidential oversight and management of the agencies listed in this branch of government? They run themselves? That claim means nothing in practice.
For an agency to be deemed “independent” turns out to mean codependency with the industries regulated, subsidized, penalized, or otherwise impacted by its operations. HUD does housing development, FDA does pharmaceuticals, DOA does farming, DOL does unions, DOE does oil and turbines, DOD does tanks and bombs, FAA does airlines, and so on It goes forever.
That’s what “independence” means in practice: total acquiescence to industrial cartels, trade groups, and behind-the-scenes systems of payola, blackmail, and graft, while the powerless among the people live with the results. This much we have learned and cannot unlearn.
That is precisely the problem that cries out for a solution. The solution of elections seems reasonable only if the people we elected actually have the authority over the thing they seek to reform.
There are criticisms of the idea of executive control of executive agencies, which is really nothing other than the system the Founders established.
First, conceding more power to the president raises fears that he will behave like a dictator, a fear that is legitimate. Partisan supporters of Trump won’t be happy when the precedent is cited to reverse Trump’s political priorities and the agencies turn on red-state voters in revenge.
That problem is solved by dismantling agency power itself, which, interestingly, is mostly what Trump’s executive orders have sought to achieve and which the courts and media have worked to stop.
Second, one worries about the return of the “spoils system,” the supposedly corrupt system by which the president hands out favors to friends in the form of emoluments, a practice the establishment of the civil service was supposed to stop.
In reality, the new system of the early 20th century fixed nothing but only added another layer, a permanent ruling class to participate more fully in a new type of spoils system that operated now under the cloak of science and efficiency.
Honestly, can we really compare the petty thievery of Tammany Hall to the global depredations of USAID?
Third, it is said that presidential control of agencies threatens to erode checks and balances. The obvious response is the organizational chart above. That happened long ago as Congress created and funded agency after agency from the Wilson to the Biden administration, all under executive control.
Congress perhaps wanted the administrative state to be an unannounced and unaccountable fourth branch, but nothing in the founding documents created or imagined such a thing.
If you are worried about being dominated and destroyed by a ravenous beast, the best approach is not to adopt one, feed it to adulthood, train it to attack and eat people, and then unleash it.
The Covid years taught us to fear the power of the agencies and those who control them not just nationally but globally. The question now is two-fold: what can be done about it and how to get from here to there?
Trump’s executive order on the Department of Education illustrates the point precisely. His administration is so uncertain of what it does and can control, even of agencies that are wholly executive agencies, listed clearly under the heading of executive agencies, that it has to dodge and weave practical and legal barriers and land mines, even in its own supposed executive pronouncements, even to urge what might amount to be minor reforms.
Whoever is in charge of such a system, it is clearly not the people.
Author

From the Brownstone Institute
By
“People are reacting because they hear things about me that aren’t true, characterizations of things I have said that are simply not true. When they hear what I have to say, actually, about vaccines, everybody supports it.”
Robert F. Kennedy, Jr. has been confirmed as Secretary of the US Department of Health and Human Services.
Within hours, my news feed was populated with angsty articles hand-wringing about the future of vaccines under Kennedy, whom legacy media and the establishment are certain would confiscate life-saving vaccine programs, raising the spectre of mass waves of illness and death.
In particular, this quote from Senator Mitch McConnell (R-KY), the only Republican who voted against Kennedy’s confirmation, appeared over and over again:
“I’m a survivor of childhood polio. In my lifetime, I’ve watched vaccines save millions of lives from devastating diseases across America and around the world. I will not condone the re-litigation of proven cures, and neither will millions of Americans who credit their survival and quality of life to scientific miracles.”
Yet, I could not find one piece of mainstream coverage of this quote that mentioned the astonishing fact that 98% of polio cases in 2023, the most recent year for which we have full data, were caused by the polio vaccine.
You read that correctly. In 2023, 12 wild polio cases were recorded (six in Afghanistan, six in Pakistan), with a further 524 circulating vaccine-derived cases, mostly throughout Africa. This trend is in keeping with data from the previous several years.
An important contextualising detail, wouldn’t you think?

The cause of this polio resurgence is that the world’s poor are given the oral polio vaccine (OPV), which contains a weakened virus that can replicate in the gut and spread in feces, causing vaccine-derived outbreaks.
People in rich countries get the inactivated polio vaccine (IPV), which does not contain live virus and therefore does not carry the risk of spreading the very disease it’s vaccinating against.
The World Health Organization (WHO) and vaccine-promoting organisations say that the way out of the problem is to vaccinate harder, as the argument goes that outbreaks only occur in under-vaccinated communities.
This may be well and good, but the total omission of the fact from media coverage that the goalposts have shifted from eradicating wild polio (not yet complete but nearly there, according to the WHO) to eradicating vaccine-derived polio (the main problem these days) underscores that this is why hardly anyone who knows anything trusts the media anymore.
A member of my extended family has polio. It’s nasty and life-altering and I wouldn’t wish it on anyone.
That’s why I would hope that any vaccines given would be safe – contracting polio from the supposedly preventative vaccine is the worst-case scenario, second only to death.
This is Kennedy’s expressly stated aim.
“When people actually hear what I think about vaccines, which is common sense, which is vaccines should be tested, they should be safe, everyone should have informed consent,” he said at his confirmation press conference.
“People are reacting because they hear things about me that aren’t true, characterisations of things I have said that are simply not true.
“When they hear what I have to say, actually, about vaccines, everybody supports it.”
Grown-ups who support vaccines can walk and chew gum. From the point of view of the public health establishment, the polio vaccine has prevented millions of cases and has nearly eradicated the disease.
At the same time, the world’s poorest are afflicted with polio outbreaks which we can work to prevent, and the safety of all polio vaccine products on the market should be subject to the rigorous standards applied to all other medicines.
Unless you think that poor people don’t matter, in which case the status quo might suit you fine.
Republished from the author’s Substack
Author



Province introducing “Patient-Focused Funding Model” to fund acute care in Alberta

Mark Carney To Ban Free Speech if Elected

Musk Slashes DOGE Savings Forecast By 85%
What Trump Says About Modern U.S. And What Carney Is Hiding About Canada

Taxpayers urge federal party leaders to drop home sale reporting to CRA
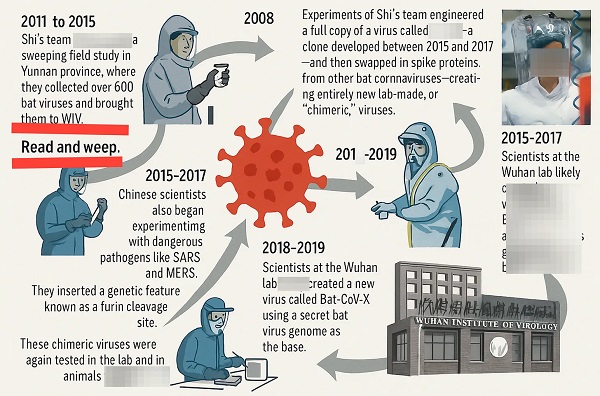
BLOCKBUSTER REPORT: Canada’s ties to Wuhan Institute of Virology and creation of COVID uncovered by Sam Cooper of The Bureau

Trump targets Washington’s climate laws in recent executive order
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoNeil Young + Carney / Freedom Bros
-
 Business1 day ago
Business1 day agoDOGE Is Ending The ‘Eternal Life’ Of Government
-
 espionage17 hours ago
espionage17 hours agoEx-NYPD Cop Jailed in Beijing’s Transnational Repatriation Plot, Canada Remains Soft Target
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoRCMP Whistleblowers Accuse Members of Mark Carney’s Inner Circle of Security Breaches and Surveillance
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoTucker Carlson Interviews Maxime Bernier: Trump’s Tariffs, Mass Immigration, and the Oncoming Canadian Revolution
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoCanada drops retaliatory tariffs on automakers, pauses other tariffs
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoBureau Exclusive: Chinese Election Interference Network Tied to Senate Breach Investigation
-
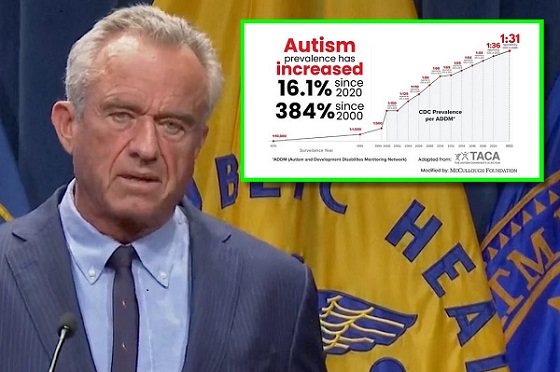 Autism2 days ago
Autism2 days agoRFK Jr. Exposes a Chilling New Autism Reality