Fraser Institute
Enough talk, we need to actually do something about Canadian health care


From the Macdonald Laurier Institute
By J. Edward Les for Inside Policy

Canada spends more on health care as a percentage of GDP than almost all other OECD countries, yet we rank behind most of them when it comes to outcomes that matter.
I drove a stretch of road near Calgary’s South Health Campus the other day, a section with a series of three intersections in a span of less than a few hundred metres. That is, I tried to drive it – but spent far more time idling than moving.
At each intersection, after an interminable wait, the light turned green just as the next one flipped to red, grinding traffic to a halt just after it got rolling. It was excruciating; I’m quite sure I spied a snail on crutches racing by – no doubt making a beeline (snail-line?) for the ER a stone’s throw away.
The street’s sluggishness is perhaps reflective of the hospital next to it, given that our once-cherished universal health care system has crumbled into a universal waiting system – a system seemingly crafted (like that road) to obstruct flow rather than enable it. In fact, the pace of medical care delivery in this country has become so glacial that even a parking lot by comparison feels like the Indianapolis Speedway.
The health care crisis grows more dire by the day. Reforms are long overdue. Canada spends more on health care as a percentage of GDP than almost all other OECD countries, yet we rank behind most of them when it comes to outcomes that matter.
And we’re paying with our lives: according to the Canadian Institute for Health Information, thousands of Canadians die each and every year because of the inefficiencies of our system.
Yet for all that we are paralyzed by the enormity and complexity of the mushrooming disaster. We talk about solutions – and then we talk and talk some more. But for all the talking, precious little action is taken.
I’m reminded of an Anne Lamotte vignette, related in her bestselling book Bird By Bird:
Thirty years ago my older brother, who was ten years old at the time, was trying to get a report written on birds that he’d had three months to write, which was due the next day. We were out at our family cabin in Bolinas, and he was at the kitchen table close to tears, surrounded by binder paper and pencils and unopened books about birds, immobilized by the hugeness of the task ahead. Then my father sat down beside him, put his arm around my brother’s shoulder, and said, “Bird by bird, buddy. Just take it bird by bird.”
So it is with Canadian health care: we’ve wasted years wringing our hands about the woeful state of affairs, while doing precious little about it.
Enough procrastinating. It’s time to tackle the crisis, bird by bird.
One thing we can do is to let doctors be doctors. A few weeks ago, in a piece titled “Should Doctors Mind Their Own Business?”, I questioned the customary habit of doctors hanging out their shingles in small independent community practices. Physicians spend long years of training to master their craft, years during which they receive no training in business methods whatsoever, and then we expect them to master those skills off to the side of their exam rooms. Some do it well, but many do not – and it detracts from their attention to patients.
We don’t install newly minted teachers in classrooms and at the same time task them with the keeping the lights on, managing the supply chain, overseeing staffing and payroll, and all the other mechanics of running schools. Why do we expect that of doctors?
Keeping doctors embedded within large, expensive, inefficient, bureaucracy-choked hospitals isn’t the solution, either.
There’s a better way, I argued in my essay: regional medical centres – centres built and administered in partnership with the private sector.
Such centres would allow practitioners currently practicing in the community to ply their trade unencumbered by the nuts and bolts of running a business; and they would allow us to decant a host of services from hospitals, which should be reserved for what only hospitals can do: emergency services, inpatient care, surgeries, and the like.
In short, we should let doctors be doctors, and hospitals be hospitals.
To garner feedback, I dumped my musings into a couple of online physician forums to which I belong, tagged with the query: “Food for thought, or fodder for the compost bin?”
The verdict? Hands down, the compost bin.
I was a bit taken aback, initially. Offended, even – because who among us isn’t in love with their own ideas?
But it quickly became evident from my peers’ comments that I’d been misunderstood. Not because my doctor friends are dim, but because I hadn’t been clear.
When I proposed in my essay that we “leave the administration and day-to-day tasks of running those centres to business folks who know what they’re doing,” my colleagues took that to mean that doctors would be serving at the beck and call of a tranche of ill-informed government-enabled administrators – and they reacted to the notion with anaphylactic derision. And understandably so: too many of us have long and painful experience with thick layers of health care bureaucracy seemingly organized according to the Peter Principle, with people promoted to – and permanently stuck at – the level of their incompetence.
But I didn’t mean to suggest – not for a minute – that doctors shouldn’t be engaged in running these centres. I also wrote: “None of which is to suggest that doctors shouldn’t be involved, by aptitude and inclination, in influencing the set-up and management of regional centres – of course, they should.”
Of course they should. There are plenty of physicians equipped with both the skills and interest needed to administer these centres; and they should absolutely be front and centre in leading them.
But more than that: everyone should have skin in the game. All workers have the right to share in the success of an enterprise; and when they do, everybody wins. When everyone is pulling in the same direction because everyone shares in the wins, waste and inefficiencies are rooted out like magic.
Contrast that to how hospitals are run, with scarcely anyone aware of the actual cost of the blood tests or CT scans they order or the packets of suture and gauze they rip open, and with the motivations of administrative staff, nurses, doctors, and other personnel running off in more directions than a flock of headless chickens. The capacity for waste and inefficiencies is almost limitless.
I don’t mean to suggest that the goal of regional medical centres should be to turn a profit; but fiscal prudence and economic accountability are to be celebrated, because money not wasted is money that can be allocated to enhancing patient care.
Nor do I mean to intimate that sensible resource management should be the only parameter tracked; patient outcomes and patient satisfaction are paramount.
What should government’s role be in all this? Initially, to incentivize the creation of these centres via public-private partnerships; and then, crucially, to encourage competition among them and to reward innovation and performance, with optimization of the three key metrics – patient outcomes, patient satisfaction, and economic accountability – always in focus.
No one should be mandated to work in non-hospital regional medical centres. It’s a free country (or it should be): doctors should be free to hang out their own community shingles if they wish. But if we build the model correctly, my contention is that most medical professionals will prefer to work collaboratively under one roof with a diverse group of colleagues, unencumbered by the mundanities of running a business, but also free of choking hospital bureaucracy.
I connected a couple weeks ago with the always insightful economist Jack Mintz (who is also a distinguished fellow at the Macdonald-Laurier Institute). Mintz sits on the board of a Toronto-area hospital and sees first-hand “the problems with the lack of supply, population growth, long wait times between admission and getting a bed, emergency room overuse,” and so on.
“Something has to give,” he said. “Probably more resources but better managed. We really need major reform.”
On that we can all agree. We can’t carry on this way.
So, let’s stop idling; and let’s green-light some fixes.
As Samwise Gamgee said in The Lord of the Rings, “It’s the job that’s never started as takes longest to finish.”
Dr. J. Edward Les is a pediatrician in Calgary who writes on politics, social issues, and other matters.

From the Fraser Institute
According to a recent study, living standards in Canada have declined over the past five years. And the country’s economic growth has been “ugly.” Crucially, all 10 provinces are experiencing this economic stagnation—there are no exceptions to Canada’s “ugly” growth record. In 2026, reversing this trend should be the top priority for the Carney government and provincial governments across the country.
Indeed, demographic and economic data across the country tell a remarkably similar story over the past five years. While there has been some overall economic growth in almost every province, in many cases provincial populations, fuelled by record-high levels of immigration, have grown almost as quickly. Although the total amount of economic production and income has increased from coast to coast, there are more people to divide that income between. Therefore, after we account for inflation and population growth, the data show Canadians are not better off than they were before.
Let’s dive into the numbers (adjusted for inflation) for each province. In British Columbia, the economy has grown by 13.7 per cent over the past five years but the population has grown by 11.0 per cent, which means the vast majority of the increase in the size of the economy is likely due to population growth—not improvements in productivity or living standards. In fact, per-person GDP, a key indicator of living standards, averaged only 0.5 per cent per year over the last five years, which is a miserable result by historic standards.
A similar story holds in other provinces. Prince Edward Island, Nova Scotia, Quebec and Saskatchewan all experienced some economic growth over the past five years but their populations grew at almost exactly the same rate. As a result, living standards have barely budged. In the remaining provinces (Newfoundland and Labrador, New Brunswick, Ontario, Manitoba and Alberta), population growth has outstripped economic growth, which means that even though the economy grew, living standards actually declined.
This coast-to-coast stagnation of living standards is unique in Canadian history. Historically, there’s usually variation in economic performance across the country—when one region struggles, better performance elsewhere helps drive national economic growth. For example, in the early 2010s while the Ontario and Quebec economies recovered slowly from the 2008/09 recession, Alberta and other resource-rich provinces experienced much stronger growth. Over the past five years, however, there has not been a “good news” story anywhere in the country when it comes to per-person economic growth and living standards.
In reality, Canada’s recent record-high levels of immigration and population growth have helped mask the country’s economic weakness. With more people to buy and sell goods and services, the overall economy is growing but living standards have barely budged. To craft policies to help raise living standards for Canadian families, policymakers in Ottawa and every provincial capital should remove regulatory barriers, reduce taxes and responsibly manage government finances. This is the great policy challenge for governments across the country in 2026 and beyond.

Ben Eisen
Senior Fellow, Fraser Institute

Jake Fuss
Director, Fiscal Studies, Fraser Institute

From the Fraser Institute
The dawn of a new year is an opportune time to ponder the recent performance of Canada’s $3.4 trillion economy. And the overall picture is not exactly cheerful.
Since the start of 2025, our principal trading partner has been ruled by a president who seems determined to unravel the post-war global economic and security order that provided a stable and reassuring backdrop for smaller countries such as Canada. Whether the Canada-U.S.-Mexico trade agreement (that President Trump himself pushed for) will even survive is unclear, underscoring the uncertainty that continues to weigh on business investment in Canada.
At the same time, Europe—representing one-fifth of the global economy—remains sluggish, thanks to Russia’s relentless war of choice against Ukraine, high energy costs across much of the region, and the bloc’s waning competitiveness. The huge Chinese economy has also lost a step. None of this is good for Canada.
Yet despite a difficult external environment, Canada’s economy has been surprisingly resilient. Gross domestic product (GDP) is projected to grow by 1.7 per cent (after inflation) this year. The main reason is continued gains in consumer spending, which accounts for more than three-fifths of all economic activity. After stripping out inflation, money spent by Canadians on goods and services is set to climb by 2.2 per cent in 2025, matching last year’s pace. Solid consumer spending has helped offset the impact of dwindling exports, sluggish business investment and—since 2023—lacklustre housing markets.
Another reason why we have avoided a sharper economic downturn is that the Trump administration has, so far, exempted most of Canada’s southbound exports from the president’s tariff barrage. This has partially cushioned the decline in Canada’s exports—particularly outside of the steel, aluminum, lumber and auto sectors, where steep U.S. tariffs are in effect. While exports will be lower in 2025 than the year before, the fall is less dramatic than analysts expected 6 to 8 months ago.
Although Canada’s economy grew in 2025, the job market lost steam. Employment growth has softened and the unemployment rate has ticked higher—it’s on track to average almost 7 per cent this year, up from 5.4 per cent two years ago. Unemployment among young people has skyrocketed. With the economy showing little momentum, employment growth will remain muted next year.
Unfortunately, there’s nothing positive to report on the investment front. Adjusted for inflation, private-sector capital spending has been on a downward trajectory for the last decade—a long-term trend that can’t be explained by Trump’s tariffs. Canada has underperformed both the United States and several other advanced economies in the amount of investment per employee. The investment gap with the U.S. has widened steadily since 2014. This means Canadian workers have fewer and less up-to-date tools, equipment and technology to help them produce goods and services compared to their counterparts in the U.S. (and many other countries). As a result, productivity growth in Canada has been lackluster, narrowing the scope for wage increases.
Preliminary data indicate that both overall non-residential investment and business capital spending on machinery, equipment and advanced technology products will be down again in 2025. Getting clarity on the future of the Canada-U.S. trade relationship will be key to improving the business environment for private-sector investment. Tax and regulatory policy changes that make Canada a more attractive choice for companies looking to invest and grow are also necessary. This is where government policymakers should direct their attention in 2026.

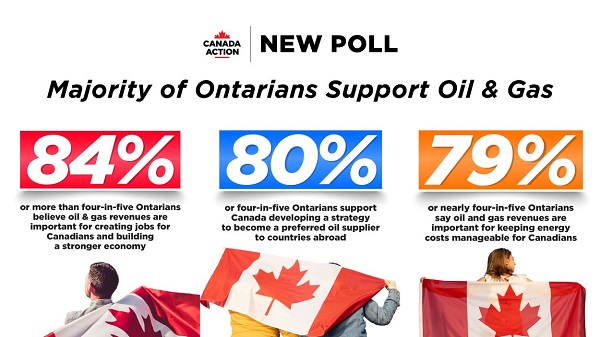
New Poll Shows Ontarians See Oil & Gas as Key to Jobs, Economy, and Trade

US Under Secretary of State Slams UK and EU Over Online Speech Regulation, Announces Release of Files on Past Censorship Efforts

Sweden Fixed What Canada Won’t Even Name

Alberta Next Panel calls for less Ottawa—and it could pay off

“Magnitude cannot be overstated”: Minnesota aid scam may reach $9 billion

Largest fraud in US history? Independent Journalist visits numerous daycare centres with no children, revealing massive scam

US Halts Construction of Five Offshore Wind Projects Due To National Security
-
Business1 day ago
Dark clouds loom over Canada’s economy in 2026
-
 Business1 day ago
Business1 day agoThe Real Reason Canada’s Health Care System Is Failing
-
 Business1 day ago
Business1 day agoFederal funds FROZEN after massive fraud uncovered: Trump cuts off Minnesota child care money
-
 Addictions1 day ago
Addictions1 day agoCoffee, Nicotine, and the Politics of Acceptable Addiction
-
 Opinion24 hours ago
Opinion24 hours agoGlobally, 2025 had one of the lowest annual death rates from extreme weather in history
-
 International8 hours ago
International8 hours agoTrump confirms first American land strike against Venezuelan narco networks
-
 Business8 hours ago
Business8 hours agoHow convenient: Minnesota day care reports break-in, records gone
-
Business7 hours ago
The great policy challenge for governments in Canada in 2026