COVID-19
71% of reported adverse reactions to COVID-19 vaccine from just 4.2% of vaccine batches: Danish study

From Dr. John Campbell on YouTube
A report “Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine” by Danish researchers Max Schmeling, Vibeke Manniche, Peter Riis Hansen is shedding light on the number of adverse reactions to specific batches of the Pfizer-BioNTech’s COVID-19 vaccines.

The researchers note in their report
“Vaccine vials with individual doses are supplied in batches with stringent quality control to ensure batch and dose uniformity.2 Clinical data on individual vaccine batch levels have not been reported and batch-dependent variation in the clinical efficacy and safety of authorized vaccines would appear to be highly unlikely. However, not least in view of the emergency use market authorization and rapid implementation of large-scale vaccination programs, the possibility of batch-dependent variation appears worthy of investigation. We therefore examined rates of SAEs between different BNT162b2 vaccine batches administered in Denmark (population 5.8 million) from 27 December 2020 to 11 January 2022.”
The results of the study are astounding. In certain vaccine batches reported adverse reactions occurred in one out of every twenty shots. Other batches have yet to be associated with any adverse reactions at all. As British health researcher Dr. John Campbell explains, this study could pose very serious questions Pfizer must address.
Viral Vaccine paper
Dr. Campbell’s presentation notes:
Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine
https://onlinelibrary.wiley.com/doi/1…
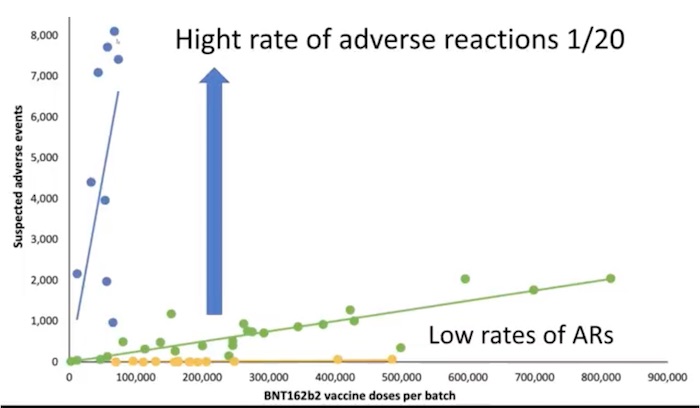
71% of the suspected adverse reactions occurred in 4.2% of the vaccine batches
Numbers of suspected adverse events (SAEs), after BNT612b2 mRNA vaccination in Denmark.
27 December 2020–11 January 2022, (population 5.8 million)
(According to the number of doses per vaccine batch)
Each dot represents a single vaccine batch.
By 11 November 2022 (European area) 701 million doses of Pfizer given 971,021 reports of suspected adverse effects (SAEs)
Clinical data on individual vaccine batch levels have not been reported (batch-dependent variation in the clinical efficacy and safety of authorized vaccines would appear to be highly unlikely)
We therefore examined rates of SAEs between different BNT162b2 vaccine batches administered in Denmark
Data on all SAE cases, Danish Medical Agency (DKMA) SAE seriousness was classified as non-serious, serious (hospitalization or prolongation of existing hospitalization, life-threatening illness, permanent disability or congenital malformation) or SAE-related d****
Anonymized data SAEs were counted on a batch level by linking individual SAEs to the batch label(s) of BNT162b dose(s)
10,793,766 doses administered 4,026,575 persons 52 different BNT162b2 vaccine batches (2,340–814,320 doses per batch)
43,496 SAEs were registered in 13,635 persons 61,847 batch-identifiable SAEs, of which 14,509 (23.5%) were classified as severe, 579 (0.9%) were SAE-related d*****
Unexpectedly Rates of SAEs per 1000 doses varied considerably between vaccine batches
From 1 SAE per 20 doses given to I in many thousands to zero
Variabilities
Vaccine manufacturing
Storage
Transportation
Clinical handling and control
Administration technique
Viral vaccine paper, Dr Vibeke Manniche

From LifeSiteNews
A judge ruled that the Ontario Court of Justice is already ‘satisfied’ with Chris Barber’s sentence and taking away his very livelihood would be ‘disproportionate.’
A Canadian judge has dismissed a demand from Canadian government lawyers to seize Freedom Convoy leader Chris Barber’s “Big Red” semi-truck.
On Friday, Ontario Court of Justice Judge Heather Perkins-McVey denied the Crown’s application seeking to forfeit Barber’s truck.
She ruled that the court is already “satisfied” with Barber’s sentence and taking away his very livelihood would be “disproportionate.”
“This truck is my livelihood,” said Barber in a press release sent to LifeSiteNews.
“Trying to permanently seize it for peacefully protesting was wrong, and I’m relieved the court refused to allow that to happen,” he added.
Criminal defense lawyer Marwa Racha Younes was welcoming of the ruling as well, stating, “We find it was the right decision in the circumstances and are happy with the outcome.”
John Carpay, president of the Justice Centre for Constitutional Freedoms (JCCF), said the decision is “good news for all Canadians who cherish their Charter freedom to assemble peacefully.”
READ: Freedom Convoy protester appeals after judge dismissed challenge to frozen bank accounts
“Asset forfeiture is an extraordinary power, and it must not be used to punish Canadians for participating in peaceful protest,” he added in the press release.
As reported recently by LifeSiteNews, the Canadian government claimed that Barber’s truck is an “offence-related property” relating to his involvement in the 2022 protests against Canada’s COVID mandates.
At this time, the court ruling ends any forfeiture proceedings for the time being, however Barber will continue to try and appeal his criminal conviction and house arrest sentence.
Barber’s truck, a 2004 Kenworth long-haul he uses for business, was a focal point in the 2022 protests. He drove it to Ottawa, where it was parked for an extended period of time, but he complied when officials asked him to move it.
On October 7, 2025, after a long trial, Ontario Court Justice Perkins-McVey sentenced Barber and Tamara Lich, the other Freedom Convoy leader, to 18 months’ house arrest. They had been declared guilty of mischief for their roles as leaders of the 2022 protest against COVID mandates, and as social media influencers.
Lich and Barber have filed appeals of their own against their house arrest sentences, arguing that the trial judge did not correctly apply the law on their mischief charges.
Government lawyers for the Crown have filed an appeal of the acquittals of Lich and Barber on intimidation charges.
The pair’s convictions came after a nearly two-year trial despite the nonviolent nature of the popular movement.

From LifeSiteNews
Protestor Evan Blackman’s legal team argues Trudeau’s Emergencies Act-based bank account freezes were punitive state action tied directly to protest participation.
A Freedom Convoy protester whose bank accounts were frozen by the Canadian government says a judge erred after his ruling did not consider the fact that the funds were frozen under the Emergencies Act, as grounds for a stay of proceedings.
In a press release sent out earlier this week, the Justice Centre for Constitutional Freedoms (JCCF) said that Freedom Convoy protestor Evan Blackman will challenge a court ruling in his criminal case via an appeal with the Ontario Superior Court of Justice.
“This case raises serious questions about how peaceful protest is treated in Canada and about the lasting consequences of the federal government’s unlawful use of the Emergencies Act,” noted constitutional lawyer Chris Fleury. “The freezing of protestors’ bank accounts was part of a coordinated effort to suppress dissent, and courts ought to be willing to scrutinize that conduct.”
Blackman was arrested on February 18, 2022, during the police crackdown on Freedom Convoy protests against COVID restrictions, which was authorized by the Emergencies Act (EA). The EA was put in place by former Prime Minister Justin Trudeau’s Liberal government, which claimed the protests were violent, despite no evidence that this was the case.
Blackman’s three bank accounts with TD Bank were frozen due to his participation in the Freedom Convoy, following a directive ordered by Trudeau.
As reported by LifeSiteNews, in November of this year, Blackman was convicted at his retrial even though he had been acquitted at his original trial. In 2023, Blackman’s “mischief” and “obstructing police” charges were dismissed by a judge due to lack of evidence and the “poor memory of a cop regarding key details of the alleged criminal offences.”
His retrial resulted in Blackman getting a conditional discharge along with 12 months’ probation and 122 hours of community service, along with a $200 victim fine surcharge.
After this, Blackman’s application for a stay of proceedings was dismissed by the court. He had hoped to have his stay of proceedings, under section 24(1) of the Charter of Rights and Freedoms, allowed. However, the judge ruled that the freezing of his bank accounts was legally not related to his arrest, and because of this, the stay of proceedings lacked standing.
The JCCF disagreed with this ruling, noting, it “stands in contrast to a Federal Court decision finding that the government’s invocation of the Emergencies Act was unreasonable and violated Canadians’ Charter rights, including those targeted by the financial measures used against Freedom Convoy protestors.”
As of press time, a hearing date has not been scheduled.
In 2024, Federal Court Justice Richard Mosley ruled that Trudeau was “not justified” in invoking the Emergencies Act.
In early 2022, the Freedom Convoy saw thousands of Canadians from coast to coast come to Ottawa to demand an end to COVID mandates in all forms. Despite the peaceful nature of the protest, Trudeau’s federal government enacted the EA in mid-February.
After the protesters were cleared out, which was achieved through the freezing of bank accounts of those involved without a court order as well as the physical removal and arrest of demonstrators, Trudeau revoked the EA on February 23, 2022.

Brown University shooter dead of apparent self-inflicted gunshot wound

Canada Hits the Brakes on Population

Ford’s EV Fiasco Fallout Hits Hard

Why is Canada paying for dairy ‘losses’ during a boom?

Alberta’s new diagnostic policy appears to meet standard for Canada Health Act compliance

Geopolitics no longer drives oil prices the way it used to

RFK Jr reversing Biden-era policies on gender transition care for minors
-
 Artificial Intelligence2 days ago
Artificial Intelligence2 days agoUK Police Pilot AI System to Track “Suspicious” Driver Journeys
-
 Business2 days ago
Business2 days agoThe “Disruptor-in-Chief” places Canada in the crosshairs
-
 Business2 days ago
Business2 days agoJudge Declares Mistrial in Landmark New York PRC Foreign-Agent Case
-
 International1 day ago
International1 day agoGeorgia county admits illegally certifying 315k ballots in 2020 presidential election
-
 Alberta1 day ago
Alberta1 day agoA Christmas wish list for health-care reform
-
 Business22 hours ago
Business22 hours agoSome Of The Wackiest Things Featured In Rand Paul’s New Report Alleging $1,639,135,969,608 In Gov’t Waste
-
 Energy22 hours ago
Energy22 hours ago‘The electric story is over’
-
 International1 day ago
International1 day agoCommunist China arrests hundreds of Christians just days before Christmas