Addictions
Does America’s ‘drug czar’ hold lessons for Canada?
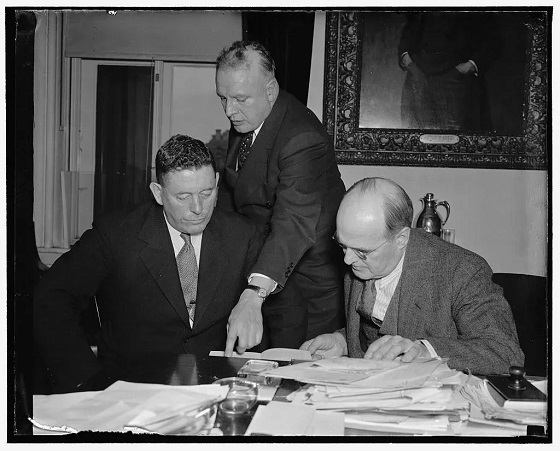
Harry Anslinger (center) discussing cannabis control with Canadian narcotics chief Charles Henry Ludovic Sharman and Assistant Secretary of the Treasury Stephen B. Gibbons in 1938. (Photo credit: United States Library of Congress’ Prints and Photographs division)

The US has had a drug czar for decades. Experts share how this position has shaped US drug policy—and what it could mean for Canada
Last week, Canada announced it would appoint a “fentanyl czar” to crack down on organized crime and border security.
The move is part of a suite of security measures designed to address US President Donald Trump’s concerns about fentanyl trafficking and forestall the imposition of 25 per cent tariffs on Canadian goods.
David Hammond, a health sciences professor and research chair at the University of Waterloo, says, “There is no question that Canada would benefit from greater leadership and co-ordination in substance use policy.”
But whether Canada’s fentanyl czar “meets these needs will depend entirely on the scope of their mandate,” he told Canadian Affairs in an email.
Canadian authorities have so far provided few details about the fentanyl czar’s powers and mandate.
A Feb. 4 government news release says the czar will focus on intelligence sharing and collaborating with US counterparts. Canada’s Public Safety Minister, David McGuinty, said in a Feb. 4 CNN interview that the position “will transcend any one part of the government … [It] will pull together a full Canadian national response — between our provinces, our police of local jurisdiction, and work with our American authorities.”
Canada’s approach to the position may take cues from the US, which has long had its own drug czar. Canadian Affairs spoke to several US historians of drug policy to better understand the nature and focus of this role in the US.
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
The first drug czar
The term “czar” refers to high-level officials who oversee specific policy areas and have broad authority across agencies.
Today, the US drug czar’s official title is director of the Office of National Drug Control Policy. The director is appointed by the president and responsible for advising the president and coordinating a national drug strategy.
Taleed El-Sabawi, a legal scholar and public health policy expert at Wayne State University in Detroit, Mich., said the Office of National Drug Control Policy has two branches: a law enforcement branch focused on drug supply, and a public health branch focused on demand for drugs.
“Traditionally, the supply side has been the focus and the demand side has taken a side seat,” El-Sabawi said.
David Herzberg, a historian at University at Buffalo in Buffalo, N.Y., made a similar observation.
“US drug policy has historically been dominated by moral crusading — eliminating immoral use of drugs, and policing [or] punishing the immoral people (poor, minority, and foreign/traffickers) responsible for it,” Herzberg told Canadian Affairs in an email.
Harry Anslinger, who was appointed in 1930 as the first commissioner of the Federal Bureau of Narcotics, is considered the earliest iteration of the US drug czar. The bureau later merged into the Drug Enforcement Administration, the lead federal agency responsible for enforcing US drug laws.
Anslinger prioritized enforcement, and his impact was complex.
“He was part of a movement to characterize addicts as depraved and inferior individuals and he supported punitive responses not just to drug dealing but also to drug use,” said Caroline Acker, professor emerita of history at Carnegie Mellon University in Pittsburgh, Pa.
But Anslinger also cracked down on the pharmaceutical industry. He restricted opioid production, effectively making it a low-profit, tightly controlled industry, and countered pharmaceutical public relations campaigns with his own.
“The Federal Bureau of Narcotics [at the time could] in fact be seen as the most robust national consumer protection agency, with powers to regulate and constrain major corporations that the [Food and Drug Administration] could only dream of,” said Herzberg.
The punitive approach to drugs put in place by Anslinger was the dominant model until the Nixon administration. In 1971, President Richard Nixon created an office dedicated to drug abuse prevention and appointed Jerome Jaffe as drug czar.
Jaffe established a network of methadone treatment facilities across the US. Nixon initially combined public health and law enforcement to combat rising heroin use among Vietnam War soldiers, calling addiction the nation’s top health issue.
However, Nixon later reverted back to an enforcement approach when he used drug policy to target Black communities and anti-war activists.
“We knew we couldn’t make it illegal to be either against the war or Black, but by getting the public to associate the hippies with marijuana and Blacks with heroin, and then criminalizing both heavily, we could disrupt those communities,” Nixon’s top domestic policy aide, John Ehrlichman, said in a 1994 interview.
 |
Michael Botticelli, Acting Director of the Office of National Drug Control Policy March 7, 2014 – Jan. 20, 2017 under President Barack Obama. [Photo Credit: Executive Office of the President of the United States]
Back and forth
More recently, in 2009, President Barack Obama appointed Michael Botticelli as drug czar. Botticelli was the first person in active recovery to hold the role.
The Obama administration recognized addiction as a chronic brain disease, a view already accepted in scientific circles but newly integrated into national drug policy. It reduced drug possession sentences and emphasized prevention and treatment.
Trump, who succeeded Obama in 2016, prioritized law enforcement while rolling back harm reduction. In 2018, his administration called for the death penalty for drug traffickers, and in 2019, sued to block a supervised consumption site in Philadelphia, Pa.
Trump appointed James Carroll as drug czar in 2017. But in 2018 Trump proposed slashing the office’s budget by more than 90 per cent and transferring authority for key drug programs to other agencies. Lawmakers blocked the plan, however, and the Office of National Drug Control Policy remained intact.
In 2022, President Joe Biden appointed Dr. Rahul Gupta, the first medical doctor to serve as drug czar. Herzberg says Gupta also prioritized treatment, by, for example, expanding access to naloxone and addiction medications. But he also cracked down on drug trafficking.
In December 2024, Gupta outlined America’s international efforts to combat fentanyl trafficking, naming China, Mexico, Colombia and India as key players — but not Canada.
Gupta’s last day was Jan. 19. Trump has yet to appoint someone to the role.
Canada’s fentanyl czar
El-Sabawi says she views Canada’s appointment of a drug czar as a signal that the government will be focused on supply side, law enforcement initiatives.
Hammond, the University of Waterloo professor, says he hopes efforts to address Canada’s drug problems focus on both the supply and demand sides of the equation.
“Supply-side measures are an important component of substance use policy, but limited in their effectiveness when they are not accompanied by demand-side policies,” he said.
The Canada Border Services Agency and Health Canada redirected Canadian Affairs’ inquiries about the new fentanyl czar role to Public Safety Canada. Public Safety Canada did not respond to multiple requests for comment before publication.
El-Sabawi suggests the entire drug czar role needs rethinking.
“I think the role needs to be re-envisioned as one that is more of a coordinator [across] the administrative branch on addiction and overdose issues … as opposed to what it is now, which is really a mouthpiece — symbolic,” she said.
“Most drug czars don’t get much done.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle.
Our content is always free – but if you want to help us commission more high-quality journalism, consider getting a voluntary paid subscription.
2025 Federal Election
Poilievre to invest in recovery, cut off federal funding for opioids and defund drug dens

From Conservative Party Communications
Poilievre will Make Recovery a Reality for 50,000 Canadians
Conservative Leader Pierre Poilievre pledged he will bring the hope that our vulnerable Canadians need by expanding drug recovery programs, creating 50,000 new opportunities for Canadians seeking freedom from addiction. At the same time, he will stop federal funding for opioids, defund federal drug dens, and ensure that any remaining sites do not operate within 500 meters of schools, daycares, playgrounds, parks and seniors’ homes, and comply with strict new oversight rules that focus on pathways to treatment.
More than 50,000 people have lost their lives to fentanyl since 2015—more Canadians than died in the Second World War. Poilievre pledged to open a path to recovery while cracking down on the radical Liberal experiment with free access to illegal drugs that has made the crisis worse and brought disorder to local communities.
Specifically, Poilievre will:
- Fund treatment for 50,000 Canadians. A new Conservative government will fund treatment for 50,000 Canadians in treatment centres with a proven record of success at getting people off drugs. This includes successful models like the Bruce Oake Recovery Centre, which helps people recover and reunite with their families, communities, and culture. To ensure the best outcomes, funding will follow results. Where spaces in good treatment programs exist, we will use them, and where they need to expand, these funds will allow that.
- Ban drug dens from being located within 500 metres of schools, daycares, playgrounds, parks, and seniors’ homes and impose strict new oversight rules. Poilievre also pledged to crack down on the Liberals’ reckless experiments with free access to illegal drugs that allow provinces to operate drug sites with no oversight, while pausing any new federal exemptions until evidence justifies they support recovery. Existing federal sites will be required to operate away from residential communities and places where families and children frequent and will now also have to focus on connecting users with treatment, meet stricter regulatory standards or be shut down. He will also end the exemption for fly-by-night provincially-regulated sites.
“After the Lost Liberal Decade, Canada’s addiction crisis has spiralled out of control,” said Poilievre. “Families have been torn apart while children have to witness open drug use and walk through dangerous encampments to get to school. Canadians deserve better than the endless Liberal cycle of crime, despair, and death.”
Since the Liberals were first elected in 2015, our once-safe communities have become sordid and disordered, while more and more Canadians have been lost to the dangerous drugs the Liberals have flooded into our streets. In British Columbia, where the Liberals decriminalized dangerous drugs like fentanyl and meth, drug overdose deaths increased by 200 percent.
The Liberals also pursued a radical experiment of taxpayer-funded hard drugs, which are often diverted and resold to children and other vulnerable Canadians. The Vancouver Police Department has said that roughly half of all hydromorphone seizures were diverted from this hard drugs program, while the Waterloo Regional Police Service and Niagara Regional Police Service said that hydromorphone seizures had exploded by 1,090% and 1,577%, respectively.
Despite the death and despair that is now common on our streets, bizarrely Mark Carney told a room of Liberal supporters that 50,000 fentanyl deaths in Canada is not “a crisis.” He also hand-picked a Liberal candidate who said the Liberals “would be smart to lean into drug decriminalization” and another who said “legalizing all drugs would be good for Canada.”
Carney’s star candidate Gregor Robertson, an early advocate of decriminalization and so-called safe supply, wanted drug dens imposed on communities without any consultation or public safety considerations. During his disastrous tenure as Vancouver Mayor, overdoses increased by 600%.
Alberta has pioneered an approach that offers real hope by adopting a recovery-focused model of care, leading to a nearly 40 percent reduction in drug-poisoning deaths since 2023—three times the decrease seen in British Columbia. However, we must also end the Liberal drug policies that have worsened the crisis and harmed countless lives and families.
To fund this policy, a Conservative government will stop federal funding for opioids, defund federal drug dens, and sue the opioid manufacturers and consulting companies who created this crisis in the first place.
“Canadians deserve better than the Liberal cycle of crime, despair, and death,” said Poilievre. “We will treat addiction with compassion and accountability—not with more taxpayer-funded poison. We will turn hurt into hope by shutting down drug dens, restoring order in our communities, funding real recovery, and bringing our loved ones home drug-free.”

By Adam Zivo
Sweden, the U.K., and Canada all experimented with providing opioids to addicts. The results were disastrous.
[This article was originally published in City Journal, a public policy magazine and website published by the Manhattan Institute for Policy Research. We encourage our readers to subscribe to them for high-quality analysis on urban issues]
Last August, Denver’s city council passed a proclamation endorsing radical “harm reduction” strategies to address the drug crisis. Among these was “safer supply,” the idea that the government should give drug users their drug of choice, for free. Safer supply is a popular idea among drug-reform activists. But other countries have already tested this experiment and seen disastrous results, including more addiction, crime, and overdose deaths. It would be foolish to follow their example.
The safer-supply movement maintains that drug-related overdoses, infections, and deaths are driven by the unpredictability of the black market, where drugs are inconsistently dosed and often adulterated with other toxic substances. With ultra-potent opioids like fentanyl, even minor dosing errors can prove fatal. Drug contaminants, which dealers use to provide a stronger high at a lower cost, can be just as deadly and potentially disfiguring.
Because of this, harm-reduction activists sometimes argue that governments should provide a free supply of unadulterated, “safe” drugs to get users to abandon the dangerous street supply. Or they say that such drugs should be sold in a controlled manner, like alcohol or cannabis—an endorsement of partial or total drug legalization.
But “safe” is a relative term: the drugs championed by these activists include pharmaceutical-grade fentanyl, hydromorphone (an opioid as potent as heroin), and prescription meth. Though less risky than their illicit alternatives, these drugs are still profoundly dangerous.
The theory behind safer supply is not entirely unreasonable, but in every country that has tried it, implementation has led to increased suffering and addiction. In Europe, only Sweden and the U.K. have tested safer supply, both in the 1960s. The Swedish model gave more than 100 addicts nearly unlimited access through their doctors to prescriptions for morphine and amphetamines, with no expectations of supervised consumption. Recipients mostly sold their free drugs on the black market, often through a network of “satellite patients” (addicts who purchased prescribed drugs). This led to an explosion of addiction and public disorder.
Most doctors quickly abandoned the experiment, and it was shut down after just two years and several high-profile overdose deaths, including that of a 17-year-old girl. Media coverage portrayed safer supply as a generational medical scandal and noted that the British, after experiencing similar problems, also abandoned their experiment.
While the U.S. has never formally adopted a safer-supply policy, it experienced something functionally similar during the OxyContin crisis of the 2000s. At the time, access to the powerful opioid was virtually unrestricted in many parts of North America. Addicts turned to pharmacies for an easy fix and often sold or traded their extra pills for a quick buck. Unscrupulous “pill mills” handed out prescriptions like candy, flooding communities with OxyContin and similar narcotics. The result was a devastating opioid epidemic—one that rages to this day, at a cumulative cost of hundreds of thousands of American lives. Canada was similarly affected.
The OxyContin crisis explains why many experienced addiction experts were aghast when Canada greatly expanded access to safer supply in 2020, following a four-year pilot project. They worried that the mistakes of the recent past were being made all over again, and that the recently vanquished pill mills had returned under the cloak of “harm reduction.”
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Most Canadian safer-supply prescribers dispense large quantities of hydromorphone with little to no supervised consumption. Patients can receive up to 40 eight-milligram pills per day—despite the fact that just two or three are enough to cause an overdose in someone without opioid tolerance. Some prescribers also provide supplementary fentanyl, oxycodone, or stimulants.
Unfortunately, many safer-supply patients sell or trade a significant portion of these drugs—primarily hydromorphone—in order to purchase more potent illicit substances, such as street fentanyl.
The problems with safer supply entered Canada’s consciousness in mid-2023, through an investigative report I wrote for the National Post. I interviewed 14 addiction physicians from across the country, who testified that safer-supply diversion is ubiquitous; that the street price of hydromorphone collapsed by up to 95 percent in communities where safer supply is available; that youth are consuming and becoming addicted to diverted safer-supply drugs; and that organized crime traffics these drugs.
Facing pushback, I interviewed former drug users, who estimated that roughly 80 percent of the safer-supply drugs flowing through their social circles was getting diverted. I documented dozens of examples of safer-supply trafficking online, representing tens of thousands of pills. I spoke with youth who had developed addictions from diverted safer supply and adults who had purchased thousands of such pills.
After months of public queries, the police department of London, Ontario—where safer supply was first piloted—revealed last summer that annual hydromorphone seizures rose over 3,000 percent between 2019 and 2023. The department later held a press conference warning that gangs clearly traffic safer supply. The police departments of two nearby midsize cities also saw their post-2019 hydromorphone seizures increase more than 1,000 percent.
The Canadian government quietly dropped its support for safer supply last year, cutting funding for many of its pilot programs. The province of British Columbia (the nexus of the harm-reduction movement) finally pulled back support last month, after a leaked presentation confirmed that safer-supply drugs are getting sold internationally and that the government is investigating 60 pharmacies for paying kickbacks to safer-supply patients. For now, all safer-supply drugs dispensed within the province must be consumed under supervision.
Harm-reduction activists have insisted that no hard evidence exists of widespread diversion of safer-supply drugs, but this is only because they refuse to study the issue. Most “studies” supporting safer supply are produced by ideologically driven activist-scholars, who tend to interview a small number of program enrollees. These activists also reject attempts to track diversion as “stigmatizing.”
The experiences of Sweden, the United Kingdom, and Canada offer a clear warning: safer supply is a reliably harmful policy. The outcomes speak for themselves—rising addiction, diversion, and little evidence of long-term benefit.
As the debate unfolds in the United States, policymakers would do well to learn from these failures. Americans should not be made to endure the consequences of a policy already discredited abroad simply because progressive leaders choose to ignore the record. The question now is whether we will repeat others’ mistakes—or chart a more responsible course.
Our content is always free –
but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.


Casino Days Bonus Offers Available for Players from Alberta
Is HNIC Ready For The Winnipeg Jets To Be Canada’s Heroes?

CSIS Warned Beijing Would Brand Conservatives as Trumpian. Now Carney’s Campaign Is Doing It.

No Matter The Winner – My Canada Is Gone

-
 Business1 day ago
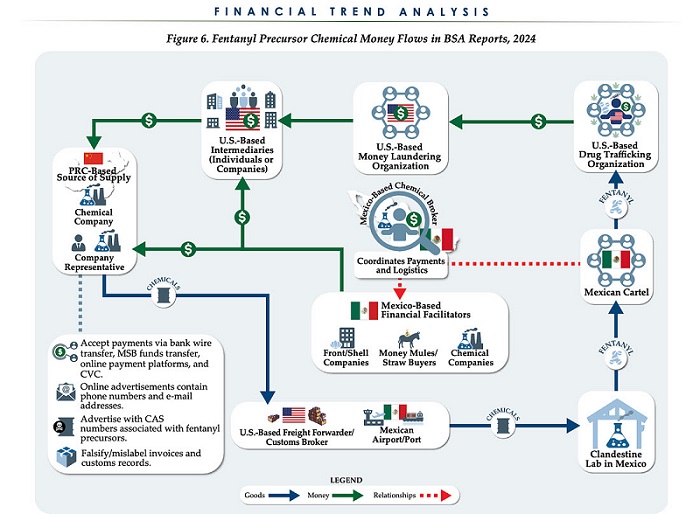
Business1 day agoChina, Mexico, Canada Flagged in $1.4 Billion Fentanyl Trade by U.S. Financial Watchdog
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoTucker Carlson Interviews Maxime Bernier: Trump’s Tariffs, Mass Immigration, and the Oncoming Canadian Revolution
-
 espionage1 day ago
espionage1 day agoEx-NYPD Cop Jailed in Beijing’s Transnational Repatriation Plot, Canada Remains Soft Target
-
 Business2 days ago
Business2 days agoDOGE Is Ending The ‘Eternal Life’ Of Government
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoBREAKING from THE BUREAU: Pro-Beijing Group That Pushed Erin O’Toole’s Exit Warns Chinese Canadians to “Vote Carefully”
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoCanada drops retaliatory tariffs on automakers, pauses other tariffs
-
 Daily Caller1 day ago
Daily Caller1 day agoTrump Executive Orders ensure ‘Beautiful Clean’ Affordable Coal will continue to bolster US energy grid
-
 Daily Caller1 day ago
Daily Caller1 day agoDOJ Releases Dossier Of Deported Maryland Man’s Alleged MS-13 Gang Ties