Brownstone Institute
Covid was Spreading Across the U.S. in 2019

If it could be proven that the virus that causes COVID-19 was spreading throughout the world by November 2019 (or even earlier), the shift in the Covid narrative might be seismic.
For example, if the virus had already infected large numbers of people, the justification for the lockdowns of mid-March 2020 to “slow or stop the spread” of a newly arrived virus would be shown to be nonsense.
Estimates of the number of people who had already developed natural immunity as well as of the infection fatality rate (IFR) might be dramatically different. It would suggest the disease was not nearly as lethal as experts proclaimed. The mass fear in the public – a prerequisite for lockdowns and later for mass vaccinations – might be much lower.
Given these points, it’s odd public health officials and investigative journalists have eschewed serious investigations that might confirm this virus had already spread around the world before January 1st, 2020.
A common-sense project to ‘prove’ early spread was occurring would be simply to test tranches of blood that were donated before the birth date of the official outbreak (December 31st 2019).
Surprisingly, however, very few antibody studies of archived blood collected before December 31st 2019 have occurred. Will Jones of The Daily Skeptic recently highlighted one such study published by researchers in France as well as a sewage study from Brazil. The first provides antibody evidence and the second RNA evidence the novel coronavirus was spreading by November 2019 in these countries.
To Will’s list, I’d add the only antibody study of archived Red Cross blood conducted by the US CDC to date. This study found 39 antibody-positive serum samples collected December 13th-16th, 2019 in California, Washington and Oregon (2% of blood samples collected from these states tested positive for antibodies).
As it takes the human body one to two weeks to produce detectable levels of antibodies, most of these 39 antibody-positive donors had been infected in November 2019 if not earlier.
For some reason, American officials performed only one antibody study of blood collected by blood bank organizations. It’s also strange that results of this study were not published until November 30th, 2020 – more than 11 months after the first tranche of archived Red Cross blood had been collected.
In a CDC press briefing held May 29th, 2020, CDC officials stated they’d searched for and could find no evidence the novel coronavirus had been “introduced” anywhere in America prior to January 20th, 2020.
I believe this statement was false, as by the time this press briefing was held, copious evidence of early spread had already been disseminated via published news accounts. For example, I’ve identified at least 17 Americans who were sick with definite Covid symptoms in November and December 2019 and all 17 had antibody evidence of prior infection. Also, all 17 of these reports were published by prominent news organizations at least 13 days before this press conference.
While a source of important evidence, antibody studies are not necessary to prove that early spread almost certainly occurred in America. Close examination of individual case histories also allows one confidently to reach this conclusion. What follows is a summary of three individual histories that lead me to conclude community spread was already occurring in America by November 2019 and probably October 2019.
For details on other American cases that date to December 2019, see this Seattle Times story and a feature story I wrote that, for some reason, was completely ignored by the mainstream press and public health officials, a fact I document in this follow-up article.
Case 1: Michael Melham of Belleville, NJ
Michael Melham, the Mayor of Belleville, NJ, was among a large group of New Jersey municipal employees who attended a conference in Atlantic City on November 19th-21st 2019. While at the conference, Melham experienced symptoms common to COVID-19.
“I was definitely feeling sick when I was there, and fought my way through it,” Mayor Melham told NJ Advance Media on April 30th, 2020.
“I have never been sicker in my entire life,” the Mayor said. “These symptoms included a 102-degree fever, chills, hallucinations and a sore throat that lasted for three weeks.” In a story published by Fox News, Mayor Melham said the illness made him feel “like a heroin addict going through withdrawals… I didn’t know what was happening to me. I never felt that I could be so sick.“
Mayor Melham felt sick enough to contact his doctor who diagnosed him with the flu. However, this diagnosis was given “over the phone” and Melham never actually received a flu test.
In late April 2020, Melham visited his doctor for his annual physical and brought up his November illness. The doctor administered an antibody test, which came back positive for Covid antibodies.
Melham later told me he actually received two positive antibody tests (previous reports mentioned just one).
“My first antibody test was a rapid test. My second was a blood test that was sent to a lab. Both were positive for the longer antibody,” Mayor Melham wrote in one email.
Mayor Melham has repeatedly made the important (if ignored) point that he tested positive for the ‘long’ (IgG) antibody. He tested negative for the IgM antibody. The presence of IgM antibodies indicate more recent infection and, per studies, these antibodies fade and are only detectable for about a month after infection.
This combination of antibody results would seem to rule out the possibility Mayor Melham experienced an asymptomatic case of Covid in the month before receiving his first antibody test. The only time Melham was sick was November 2020.
He added: “I will also tell you that since the media attention surrounding my claim, many others have come forward. I have emails from those who were actually at the same conference in Atlantic City NJ, who became just as sick as I was.”
Those who wish to gauge the credibility of the Mayor’s claims can view this four-minute YouTube interview with Mayor Melham.
I also asked Mayor Melham a question no other journalist seems to have asked him. “Did any public health official ever contact you to investigate your possible case?”
Melham’s email response: “No, nothing.”
DISCUSSION
Multiple acquaintances as well as his physician would confirm Melham was sick with symptoms common to Covid victims in November. Since he received two positive antibody tests, if the results were a false positive, he received two false positives.
As noted, Mayor Melham reports receiving emails from “multiple people… who were at the same conference who became just as sick as I was”. This would suggest the presence of community spread – a possibility which might have been confirmed if contact tracers had tested the people who’d been sick at the same conference for antibodies.
We know no public health officials contacted Mayor Melham to investigate his claim. We also know, thanks to nj.com‘s reporting, that state health officials were aware of his claim:
“Asked about the Mayor’s statements, the state health department declined comment. A spokesperson for Gov. Phil Murphy did not immediately respond to a message.”
The following points should also be emphasized. If his diagnosis had been confirmed by public health officials, Mayor Melham would have been the first known Covid case in the world, and would have been the first confirmed case in America by approximately 61 days (the first official case in America is still recorded as January 20th, 2020 – a man from Washington state who had recently returned from Wuhan).
Significantly, Mayor Melham can date the onset of his symptoms. Per numerous studies, it takes two to 14 days after infection for symptoms to manifest. This means Mayor Melham would have been infected some time between November 5th and November 19th, 2019.
Since Mayor Melham did not give the virus to himself, logic tells us the chain of transmission that ended with Michael Melham being symptomatic around November 20th, 2019 very possibly began before November 1st, 2019. This would mean that community spread was possibly occurring in New Jersey as early as October 2019.
Case 2: Uf Tukel of Delray Beach, Florida
As reported by the Palm Beach Post on May 16th, 2020:
“At least 11 people… on two small blocks alone… in a small Delray Beach (Florida) neighborhood tested positive for coronavirus antibodies in April. They felt symptoms as early as November (2019). “It didn’t have a name back then, but I have no doubt now that it was the coronavirus,” one neighbor said.”
The article names seven of these individuals and provides details and quotes about their symptoms. These seven people include Uf Tukel who was “first among (residents of the neighborhood) to feel sick in late November (2019)… For weeks, he had body aches, a severe cough and night sweats.”
While “Tukel is reluctant to say he had the coronavirus a month before Chinese officials reported the outbreak to the World Health Organisation, ‘I had all the symptoms though,’ Tukel said.”
The same logic applied to Michael Melham’s possible case would apply to Mr. Tukel’s possible case. That is, the unknown person who infected Mr. Tukel was infected earlier than Tukel, and the unknown person who infected this person contracted the virus even earlier, suggesting early spread was also happening by some point in November, if not October, in Delray Beach, Florida.
If confirmed, Mr. Tukel’s case would indicate that American cases in November were not isolated to the state of New Jersey.
Several other points included in the Post’s coverage deserve attention.
These possible Delray Beach cases include two couples, with one spouse presumably infecting the other. One child of one of these couples became infected, providing further evidence of community spread.
According to the story, none of the individuals experienced close contacts with other non-family residents of the same neighborhood. That is, there seems to be no evidence of neighbor-to-neighbor transmission.
According to the story, “all (11 individuals) recovered and haven’t been sick since.” None of the 11 had travelled to China.
Like Michael Melham, none of these 11 people tested positive for the ‘short’ (IgM) antibodies – thus none had been recently infected.
The Post article also includes this eye-opening information: “Since March (2020) about two-fifths (approximately 200, 40%) of the 500 antibody tests taken by Xera Med (a DelRay Beach private testing lab/medical clinic) have been positive, said CEO Emily Rentz.” The first two confirmed cases in Florida were recorded March 1st.
The following sentence from this article might be even more significant: “The lab shares its data on positive tests with the state health department, (Rentz) added.”
And from the same article: “The state wouldn’t say whether it is collecting antibody data from hospitals or private laboratories.”
The Post article referenced a May 5th article by the same newspaper:
“In Florida, health department reports show patients who eventually tested positive for the virus experienced symptoms as early as January. The Florida Department of Health hasn’t explained those potential fault lines in the state’s assertion that the first cases didn’t appear in Florida until March.”
The fact 40% of 500 antibody tests administered by the clinic between March and early May 2020 tested positive for Covid antibodies suggests infections were widespread in this community. And according to the CEO of this lab, these antibody results were being shared with Florida State Department of Health officials.
And apparently these weren’t the only positive antibody results that were being reported by testing labs. As reported in the same article:
The University of Miami, in randomly testing Miami-Dade County residents for antibodies, has found that the rate of infection could be 16 times higher than state data suggests, said Dr. Erin Kobetz, a professor and lead researcher on the project …
“Since first publishing her findings, Kobetz has heard from several people who shared experiences similar to the Tropic Isle neighbors… They described being sick in December and later testing positive for antibodies. They asked if what they’d experienced was COVID-19.”
Significantly, if we count possible December 2019 cases, Americans from five geographically-dispersed US states were featured in published articles. An unknown number of Americans who’ve never been featured in a newspaper article undoubtedly fit the same profile. If one adds this unknown number of never-identified people to the list of known individuals, evidence the novel coronavirus was spreading widely across America in November and December 2019 becomes even more compelling.
Not every infectious disease expert agrees with the CDC’s assessment that widespread transmission did not begin until January 20th, 2020.
“It’s possible that the disease spread as early as November,” Dr. Kobetz said.
As in New Jersey, apparently no official with the Florida Department of Health contacted any of the 11 people referenced in the Post’s article. Nor have public health officials apparently followed up with Emily Renz, CEO of Xera Med, who stated approximately 200 other local residents received positive Covid antibody tests at the clinic between March and the end of April.
Ms. Renz noted that information on all of these positive test results had been forwarded to officials at the state’s health agency. Which prompts this question: How many clinics and testing labs in America also forwarded positive antibody test results to state health agencies, agencies which presumably could and would pass this information along to their colleagues at the CDC or NIH?
What the public doesn’t know but should is how many other Americans – those with lab results not reported in the press – also tested positive for antibodies between March and early May 2020. Presumably, the CDC and state and local health agencies have these data, which have never been released to the public.
Indeed, I’ve come to believe it’s possible at least some high-ranking officials may have conspired to suppress antibody results which, if published, might have led the public to conclude this virus was spreading widely months before officials said it had been introduced in this country. Such knowledge might have changed the way tens of millions of Americans evaluated their personal Covid risk as well as their support for lockdowns.
Case 3: Shane from Marin County, California
Perhaps the first early case in America (with antibody evidence that would confirm infection) is Shane of Marin County, California. Shane’s possible early case was not featured in a newspaper article, but by Shane himself in the reader comments section that followed a May 7th 2020 New York Times story (the story describes symptoms experienced by Covid patients).
Writes Shane: “I had COVID-19 last fall, far earlier than anyone else I’ve heard of. I suspect I caught it while on an overseas trip to Italy and the Middle East – I’ve taken two antibody tests in the past month, both of which confirmed I was infected.”
As Shane recounts, he was extremely sick with signature Covid symptoms.
“For me the worst symptom by far was the dry, unproductive cough. The cough was so intense, so relentless, it left me with bruised ribs and a horrible searing pain in my chest, which also felt as if someone were sitting on it. The fever at one point reached 104.9 upon which I began hallucinating – seeing my dogs talking to me and forgetting how to open a sliding glass door. Horrible chills which led to my teeth chattering so hard my jaw ached were also another noxious gift of Covid.
“What I most remember about my experience with Covid is pain, pain from coughing, pain in my body and head, pain everywhere around me, like a smothering red blanket. At times I felt I was going to die during that week and even today I must admit I am surprised I didn’t.”
Adding credibility to his claim, Shane’s post cited two labs where he claims to have received his positive antibody tests.
“The local health centre in West Marin is where I took the latest one. The other one I took directly at the manufacturer’s location – ARCpoint Labs in Richmond. That one is only 87% accurate and not FDA approved so that’s why I took the more recent one, which was done through Quest Labs I believe.”
In the comment thread, one poster suggests it’s unlikely Shane developed Covid as there had been no reported confirmed cases from that time. This poster opines that Shane was sick with some other nasty virus and later developed an asymptomatic case of Covid. However, Shane stuck to his theory and presented reasons for his opinion.
“I suppose it’s possible but I tend to think that since what I contracted had the exact same symptoms as COVID-19 – that COVID-19 is what I had. In addition, mid-February through mid-March I was in isolation, caring for my sister who died mid-March from metastatic cervical cancer. When COVID-19 made its first appearance in the U.S. in February we very quickly put in strict isolation protocols as my sister had a compromised immune system due to chemotherapy, further insulating myself from contact and infection as well.”
Shane does not report what month he thinks he had Covid – only that it was “last fall… and far earlier than anyone else I’ve heard.” He could have been sick in November or October (maybe even late September). Shane (if he really had Covid) contracted the virus from an unknown person who would have been infected earlier than him.
Shane shared his belief he might have contracted the virus in Italy or in the Middle East, which, if true, would provide more evidence of early global spread. However, it’s also possible he contracted the virus in California.
Shane’s claim was posted in the moderated New York Times’ comments section, meaning one or more Times employees were aware of Shane’s startling claim. I imagine any Covid article, including the popular reader comments, published by the New York Times was also read by at least some employees of the CDC, NIH etc.
As only paid subscribers can make comments in the New York Times comment section, the newspaper possesses Shane’s subscription information. That is, someone at the newspaper could have easily ascertained Shane’s full name and contact information, including his street and email address.
For what it’s worth, I contacted the NY Times via its news tip email address and suggested a reporter follow up on Shane’s eye-opening claim. I did not receive a reply. This leads me to believe the New York Times is not interested in pursuing evidence of early spread in America, even in the case of a person who very well could be the first known Covid case in the world.
Conclusion
At least three Americans (either known, or in Shane’s case, easily identifiable if effort was made) possessed antibody evidence of Covid in November 2019. The infection chain that ultimately produced these symptomatic individuals likely traces to October 2019. Of note, two of these individuals received two positive antibody tests, making a false positive explanation far less likely. These cases occurred not in one state, but three states (New Jersey, Florida and California). Americans from at least 12 US states had antibody evidence of infection prior to mid-January 2020.
As far as I know, none of these 123 Americans (17 Americans identified in press reports and 106 in the Red Cross antibody study) had travelled to China. All 123 are either known or could be identified. (For unstated reasons, the CDC did not interview any of the 106 Americans who provided positive blood samples to the Red Cross.) The figure 123 does not include the unknown individuals who infected these Americans, nor does it include the possible cases that never became known to reporters or the public.
This antibody evidence strongly suggests the novel coronavirus was being transmitted person-to-person throughout the United States well before January 1st, 2020, and was probably occurring by October 2019.
If certain officials concealed this truth or were simply too incompetent to figure it out, any trust placed in such authorities is undermined. The above information also suggests that officials are not interested in conducting serious investigations into early spread of the virus, prompting a skeptic to wonder why this might be the case.
My hope is that journalists with more resources than myself, as well as officials and scientists, will belatedly and seriously investigate the strangely-ignored evidence of early spread.
This story also appeared in The Daily Skeptic.
Author


From the Brownstone Institute
By 
Who Controls the Administrative State?
President Trump on March 20, 2025, ordered the following: “The Secretary of Education shall, to the maximum extent appropriate and permitted by law, take all necessary steps to facilitate the closure of the Department of Education.”
That is interesting language: to “take all necessary steps to facilitate the closure” is not the same as closing it. And what is “permitted by law” is precisely what is in dispute.
It is meant to feel like abolition, and the media reported it as such, but it is not even close. This is not Trump’s fault. The supposed authoritarian has his hands tied in many directions, even over agencies he supposedly controls, the actions of which he must ultimately bear responsibility.
The Department of Education is an executive agency, created by Congress in 1979. Trump wants it gone forever. So do his voters. Can he do that? No but can he destaff the place and scatter its functions? No one knows for sure. Who decides? Presumably the highest court, eventually.
How this is decided – whether the president is actually in charge or really just a symbolic figure like the King of Sweden – affects not just this one destructive agency but hundreds more. Indeed, the fate of the whole of freedom and functioning of constitutional republics may depend on the answer.
All burning questions of politics today turn on who or what is in charge of the administrative state. No one knows the answer and this is for a reason. The main functioning of the modern state falls to a beast that does not exist in the Constitution.
The public mind has never had great love for bureaucracies. Consistent with Max Weber’s worry, they have put society in an impenetrable “iron cage” built of bloodless rationalism, needling edicts, corporatist corruption, and never-ending empire-building checked by neither budgetary restraint nor plebiscite.
Today’s full consciousness of the authority and ubiquity of the administrative state is rather new. The term itself is a mouthful and doesn’t come close to describing the breadth and depth of the problem, including its root systems and retail branches. The new awareness is that neither the people nor their elected representatives are really in charge of the regime under which we live, which betrays the whole political promise of the Enlightenment.
This dawning awareness is probably 100 years late. The machinery of what is popularly known as the “deep state” – I’ve argued there are deep, middle, and shallow layers – has been growing in the US since the inception of the civil service in 1883 and thoroughly entrenched over two world wars and countless crises at home and abroad.
The edifice of compulsion and control is indescribably huge. No one can agree precisely on how many agencies there are or how many people work for them, much less how many institutions and individuals work on contract for them, either directly or indirectly. And that is just the public face; the subterranean branch is far more elusive.
The revolt against them all came with the Covid controls, when everyone was surrounded on all sides by forces outside our purview and about which the politicians knew not much at all. Then those same institutional forces appear to be involved in overturning the rule of a very popular politician whom they tried to stop from gaining a second term.
The combination of this series of outrages – what Jefferson in his Declaration called “a long train of abuses and usurpations, pursuing invariably the same Object” – has led to a torrent of awareness. This has translated into political action.
A distinguishing mark of Trump’s second term has been an optically concerted effort, at least initially, to take control of and then curb administrative state power, more so than any executive in living memory. At every step in these efforts, there has been some barrier, even many on all sides.
There are at least 100 legal challenges making their way through courts. District judges are striking down Trump’s ability to fire workers, redirect funding, curb responsibilities, and otherwise change the way they do business.
Even the signature early achievement of DOGE – the shuttering of USAID – has been stopped by a judge with an attempt to reverse it. A judge has even dared tell the Trump administration who it can and cannot hire at USAID.
Not a day goes by when the New York Times does not manufacture some maudlin defense of the put-upon minions of the tax-funded managerial class. In this worldview, the agencies are always right, whereas any elected or appointed person seeking to rein them in or terminate them is attacking the public interest.
After all, as it turns out, legacy media and the administrative state have worked together for at least a century to cobble together what was conventionally called “the news.” Where would the NYT or the whole legacy media otherwise be?
So ferocious has been the pushback against even the paltry successes and often cosmetic reforms of MAGA/MAHA/DOGE that vigilantes have engaged in terrorism against Teslas and their owners. Not even returning astronauts from being “lost in space” has redeemed Elon Musk from the wrath of the ruling class. Hating him and his companies is the “new thing” for NPCs, on a long list that began with masks, shots, supporting Ukraine, and surgical rights for gender dysphoria.
What is really at stake, more so than any issue in American life (and this applies to states around the world) – far more than any ideological battles over left and right, red and blue, or race and class – is the status, power, and security of the administrative state itself and all its works.
We claim to support democracy yet all the while, empires of command-and-control have arisen among us. The victims have only one mechanism available to fight back: the vote. Can that work? We do not yet know. This question will likely be decided by the highest court.
All of which is awkward. It is impossible to get around this US government organizational chart. All but a handful of agencies live under the category of the executive branch. Article 2, Section 1, says: “The executive Power shall be vested in a President of the United States of America.”

Does the president control the whole of the executive branch in a meaningful way? One would think so. It’s impossible to understand how it could be otherwise. The chief executive is…the chief executive. He is held responsible for what these agencies do – we certainly blasted away at the Trump administration in the first term for everything that happened under his watch. In that case, and if the buck really does stop at the Oval Office desk, the president must have some modicum of control beyond the ability to tag a marionette to get the best parking spot at the agency.
What is the alternative to presidential oversight and management of the agencies listed in this branch of government? They run themselves? That claim means nothing in practice.
For an agency to be deemed “independent” turns out to mean codependency with the industries regulated, subsidized, penalized, or otherwise impacted by its operations. HUD does housing development, FDA does pharmaceuticals, DOA does farming, DOL does unions, DOE does oil and turbines, DOD does tanks and bombs, FAA does airlines, and so on It goes forever.
That’s what “independence” means in practice: total acquiescence to industrial cartels, trade groups, and behind-the-scenes systems of payola, blackmail, and graft, while the powerless among the people live with the results. This much we have learned and cannot unlearn.
That is precisely the problem that cries out for a solution. The solution of elections seems reasonable only if the people we elected actually have the authority over the thing they seek to reform.
There are criticisms of the idea of executive control of executive agencies, which is really nothing other than the system the Founders established.
First, conceding more power to the president raises fears that he will behave like a dictator, a fear that is legitimate. Partisan supporters of Trump won’t be happy when the precedent is cited to reverse Trump’s political priorities and the agencies turn on red-state voters in revenge.
That problem is solved by dismantling agency power itself, which, interestingly, is mostly what Trump’s executive orders have sought to achieve and which the courts and media have worked to stop.
Second, one worries about the return of the “spoils system,” the supposedly corrupt system by which the president hands out favors to friends in the form of emoluments, a practice the establishment of the civil service was supposed to stop.
In reality, the new system of the early 20th century fixed nothing but only added another layer, a permanent ruling class to participate more fully in a new type of spoils system that operated now under the cloak of science and efficiency.
Honestly, can we really compare the petty thievery of Tammany Hall to the global depredations of USAID?
Third, it is said that presidential control of agencies threatens to erode checks and balances. The obvious response is the organizational chart above. That happened long ago as Congress created and funded agency after agency from the Wilson to the Biden administration, all under executive control.
Congress perhaps wanted the administrative state to be an unannounced and unaccountable fourth branch, but nothing in the founding documents created or imagined such a thing.
If you are worried about being dominated and destroyed by a ravenous beast, the best approach is not to adopt one, feed it to adulthood, train it to attack and eat people, and then unleash it.
The Covid years taught us to fear the power of the agencies and those who control them not just nationally but globally. The question now is two-fold: what can be done about it and how to get from here to there?
Trump’s executive order on the Department of Education illustrates the point precisely. His administration is so uncertain of what it does and can control, even of agencies that are wholly executive agencies, listed clearly under the heading of executive agencies, that it has to dodge and weave practical and legal barriers and land mines, even in its own supposed executive pronouncements, even to urge what might amount to be minor reforms.
Whoever is in charge of such a system, it is clearly not the people.
Author


From the Brownstone Institute
What War Means
My mother once told me how my father still woke up screaming in the night years after I was born, decades after the Second World War (WWII) ended. I had not known – probably like most children of those who fought. For him, it was visions of his friends going down in burning aircraft – other bombers of his squadron off north Australia – and to be helpless, watching, as they burnt and fell. Few born after that war could really appreciate what their fathers, and mothers, went through.
Early in the movie Saving Private Ryan, there is an extended D-Day scene of the front doors of the landing craft opening on the Normandy beaches, and all those inside being torn apart by bullets. It happens to one landing craft after another. Bankers, teachers, students, and farmers being ripped in pieces and their guts spilling out whilst they, still alive, call for help that cannot come. That is what happens when a machine gun opens up through the open door of a landing craft, or an armored personnel carrier, of a group sent to secure a tree line.
It is what a lot of politicians are calling for now.
People with shares in the arms industry become a little richer every time one of those shells is fired and has to be replaced. They gain financially, and often politically, from bodies being ripped open. This is what we call war. It is increasingly popular as a political strategy, though generally for others and the children of others.
Of course, the effects of war go beyond the dismembering and lonely death of many of those fighting. Massacres of civilians and rape of women can become common, as brutality enables humans to be seen as unwanted objects. If all this sounds abstract, apply it to your loved ones and think what that would mean.
I believe there can be just wars, and this is not a discussion about the evil of war, or who is right or wrong in current wars. Just a recognition that war is something worth avoiding, despite its apparent popularity amongst many leaders and our media.
The EU Reverses Its Focus
When the Brexit vote determined that Britain would leave the European Union (EU), I, like many, despaired. We should learn from history, and the EU’s existence had coincided with the longest period of peace between Western European States in well over 2,000 years.
Leaving the EU seemed to be risking this success. Surely, it is better to work together, to talk and cooperate with old enemies, in a constructive way? The media, and the political left, center, and much of the right seemed at that time, all of nine years ago, to agree. Or so the story went.
We now face a new reality as the EU leadership scrambles to justify continuing a war. Not only continuing, but they had been staunchly refusing to even countenance discussion on ending the killing. It has taken a new regime from across the ocean, a subject of European mockery, to do that.
In Europe, and in parts of American politics, something is going on that is very different from the question of whether current wars are just or unjust. It is an apparent belief that advocacy for continued war is virtuous. Talking to leaders of an opposing country in a war that is killing Europeans by the tens of thousands has been seen as traitorous. Those proposing to view the issues from both sides are somehow “far right.”
The EU, once intended as an instrument to end war, now has a European rearmament strategy. The irony seems lost on both its leaders and its media. Arguments such as “peace through strength” are pathetic when accompanied by censorship, propaganda, and a refusal to talk.
As US Vice-President JD Vance recently asked European leaders, what values are they actually defending?
Europe’s Need for Outside Help
A lack of experience of war does not seem sufficient to explain the current enthusiasm to continue them. Architects of WWII in Europe had certainly experienced the carnage of the First World War. Apart from the financial incentives that human slaughter can bring, there are also political ideologies that enable the mass death of others to be turned into an abstract and even positive idea.
Those dying must be seen to be from a different class, of different intelligence, or otherwise justifiable fodder to feed the cause of the Rules-Based Order or whatever other slogan can distinguish an ‘us’ from a ‘them’…While the current incarnation seems more of a class thing than a geographical or nationalistic one, European history is ripe with variations of both.
Europe appears to be back where it used to be, the aristocracy burning the serfs when not visiting each other’s clubs. Shallow thinking has the day, and the media have adapted themselves accordingly. Democracy means ensuring that only the right people get into power.
Dismembered European corpses and terrorized children are just part of maintaining this ideological purity. War is acceptable once more. Let’s hope such leaders and ideologies can be sidelined by those beyond Europe who are willing to give peace a chance.
There is no virtue in the promotion of mass death. Europe, with its leadership, will benefit from outside help and basic education. It would benefit even further from leadership that values the lives of its people.
Author



The Federal Brief That Should Sink Carney
How Canada’s Mainstream Media Lost the Public Trust

Ottawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election

CBC retracts false claims about residential schools after accusing Rebel News of ‘misinformation’

-
2025 Federal Election1 day ago
The Federal Brief That Should Sink Carney
-
2025 Federal Election1 day ago
How Canada’s Mainstream Media Lost the Public Trust
-
2025 Federal Election2 days ago
Ottawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
Media14 hours ago
CBC retracts false claims about residential schools after accusing Rebel News of ‘misinformation’
-
 John Stossel1 day ago
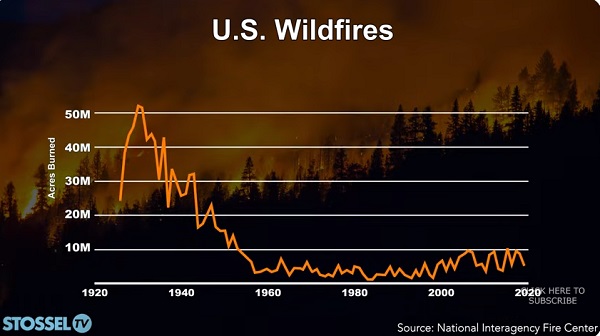
John Stossel1 day agoClimate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoReal Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
 COVID-191 day ago
COVID-191 day agoNearly Half of “COVID-19 Deaths” Were Not Due to COVID-19 – Scientific Reports Journal
-
 Bjorn Lomborg13 hours ago
Bjorn Lomborg13 hours agoNet zero’s cost-benefit ratio is CRAZY high