COVID-19
UK study of children shows heart inflammation develops after COVID vaccination, not infection
From LifeSiteNews
Researchers at Oxford University found that ‘all myocarditis and pericarditis events during the study period occurred in vaccinated individuals’ and no deaths resulted from myocarditis or pericarditis.
A new medical study conducted by researchers at Oxford University shows that the heart diseases myocarditis and pericarditis only occur after COVID-19 vaccination, not after infection, in children and adolescents.
The study, which has been published in its preprint version (before peer review), compared medical data from more than one million vaccinated and unvaccinated children ages 5 to 11 and adolescents ages 12 to 15 in England. The health of the unvaccinated children and adolescents were compared with that of those who received one and two doses of COVID-19 vaccines.
According to the study, “Whilst rare, all myocarditis and pericarditis events during the study period occurred in vaccinated individuals,” while no deaths resulted in children or adolescents from myocarditis or pericarditis.
The study also stated that “COVID-19-related hospitalization, and critical care attendance were rare in both adolescents and children and there were no COVID-19 related deaths.”
Analyzing data provided by the National Health Service (NHS), England’s OpenSAFELY-TPP database, which includes 40 percent of English primary care providers, researchers matched vaccinated and unvaccinated adolescents and children of similar relevant backgrounds — age, sex, location — charting 20 weeks for comparison of such things as positive COVID-19 tests, hospitalizations, critical care, adverse events, and non-COVID hospitalizations.
The analysis showed that myocarditis and pericarditis occurred only in vaccinated children and adolescents, with a higher incidence of both in adolescents rather than children.
Out of the more than 839,000 vaccinated children and adolescents examined in the study, 15 cases of pericarditis and three cases of myocarditis were found. All cases of myocarditis and 12 of the 15 cases of pericarditis occurred among adolescents.
Among the cases of pericarditis, all but three occurred after the first COVID vaccine dose, with more than half of the adolescents with either pericarditis and myocarditis hospitalized or taken to the ER.
The study also indicated that there was no significant difference in the severity of COVID-19 infection between vaccinated and unvaccinated children.
RELATED: Japanese study finds ‘significant increases’ in cancer deaths after third mRNA COVID doses
In comments on the new study, cardiologist Dr. Peter McCullough is reported to have stated that it is “one of many demonstrating that COVID-19 vaccination is not medically necessary for children, given the less than 1 percent rate of infection, and that excessive testing for COVID-19 is a waste of resources.”
McCullough also said, “The fact that COVID-19 vaccination can lead to side effects like myocarditis and pericarditis means it can potentially result in fatal cardiac arrest in a fraction of victims, which cannot be predicted ahead of time.”
A significant body of evidence links significant risks to the COVID vaccines, which were developed and reviewed in a fraction of the time vaccines usually take under former U.S. President Donald Trump’s Operation Warp Speed initiative. Among these risks, the U.S. federal Vaccine Adverse Event Reporting System (VAERS) reports 37,382 deaths, 215,734 hospitalizations, 21,616 heart attacks, and 28,299 myocarditis and pericarditis cases as of March 29, among other ailments.
U.S. Centers for Disease Control & Prevention (CDC) researchers have recognized a “high verification rate of reports of myocarditis to VAERS after mRNA-based COVID-19 vaccination,” leading to the conclusion that “under-reporting is more likely” than over-reporting).
An analysis of 99 million people across eight countries published in February in the journal Vaccine – the largest analysis to date – “observed significantly higher risks of myocarditis following the first, second and third doses” of mRNA-based COVID vaccines, as well as signs of increased risk of “pericarditis, Guillain-Barré syndrome, and cerebral venous sinus thrombosis,” and other “potential safety signals that require further investigation.”
In April, the CDC was forced to release by court order 780,000 previously undisclosed reports of serious adverse reactions.

From LifeSiteNews
Dr. Theresa Tam received the Order of Canada for her controversial COVID-19 response as the nation’s chief public health officer.
Canada’s former top medical advisor, known for her promotion of masking and COVID vaccines, has received one of Canada’s highest honors.
On June 30, Governor General Mary Simon awarded Dr. Theresa Tam, Canada’s former Chief Public Health Officer (CPHO), the Order of Canada award for her work implementing dangerous COVID regulations, including masking and experimental COVID shots.
“For decades, Theresa Tam has striven to advance global and national public health as a pediatric infectious disease specialist and public servant,” the press release read.
“Her tenure as Canada’s chief public health officer has been characterized by her commitment to health equity and highlighted by her leadership role in the country’s response to the COVID-19 pandemic,” it continued.
The award, given to Canadians who have made extraordinary contributions to the nation, is Canada’s second-highest civilian honor.
Tam’s reception of the award comes just weeks after she stepped down as CPHO, ending her eight-year tenure in the position.
In the early months of 2020, Tam became well-known by Canadians for leading the country’s response to the COVID “pandemic” and pushing arbitrary and dangerous regulations.
Initially, Tam assured Canadians that masking was unnecessary, ineffective, and could even pose health threats.
However, shortly after, Tam changed her policy, telling Canadians that they should even wear masks during sex, a practice which has not been proven to be effective in preventing the spread of COVID and can cause myriad health issues.
Additionally, Tam promoted experimental COVID vaccines for Canadians as young as six months old despite having no long-term studies on its effects and an extensive amount of research proving the dangers of the experimental COVID mRNA jabs that include heart damage and blood clots.
In 2022, after thousands of Canadians reported adverse effects from the vaccine, Tam announced that the federal government was reviewing all federal COVID vaccine mandates, claiming that Canada’s Public Health Agency has never outright endorsed mandatory vaccination.
Tam’s remarks come after more than 1,000 federal workers have been suspended without pay because they chose not to get the COVID jabs or disclose whether they had them per the Privacy Act.
The Order of Canada was also awarded to British Columbia Provincial Health Officer Bonnie Henry, who is known not only for her heavy-handed COVID response, but also for promoting drug use throughout the province.
In 2023, hundreds of British Columbia health care workers sued Henry for ongoing COVID shot mandates preventing them from working. Under Henry, vaccine passports were implemented which required residents to show digital proof of vaccination to enter gyms, restaurants, and other “non-essential” facilities.
Henry also pushed the experimental and dangerous vaccine on children as young as five, despite that fact that clinical trials would not be completed for another two years.
Additionally, in 2024, Henry recommended that British Columbia expand its “safe supply” program to legalize fentanyl and heroin, despite evidence that the program is not working and has worsened the provinces drug crises.


Here’s what the numbers reveal, and what it could mean for humanity
What was once dismissed as a “conspiracy theory” now has hard data behind it.
A new peer-reviewed study out of the Czech Republic has uncovered a disturbing trend: in 2022, women vaccinated against COVID-19 had 33% FEWER successful conceptions per 1,000 women compared to those who were unvaccinated.
A “successful conception” means a pregnancy that led to a live birth nine months later.
The study wasn’t small. It analyzed data from 1.3 million women aged 18 to 39.
Here’s what the numbers reveal, and what it could mean for humanity.
First, let’s talk about the study.
It was published by Manniche and colleagues in the International Journal of Risk & Safety in Medicine, a legitimate, peer-reviewed journal respected for its focus on patient safety and pharmacovigilance.
 |
The study was conducted from January 2021 to December 2023 and examined 1.3 million women aged 18–39. By the end of 2021, approximately 70% of them had received at least one COVID-19 vaccination, with 96% of the vaccinated cohort having received either the Pfizer or Moderna vaccine.
 |
By 2022, a stark difference was clear.
The vaccinated cohort averaged around 4 successful conceptions per 1,000 women per month.
That’s a staggering 33% LESS than the 6 per 1,000 seen in the unvaccinated group.
 |
This means that for every 2 vaccinated women who successfully conceived and delivered a baby, 3 unvaccinated women did the same.
In 2022, unvaccinated women were 1.5 times MORE likely to have a successful conception.
Again, that’s a conception that led to a live birth nine months later.
 |
The authors did not jump to the conclusion that their study proved causation. They cited that other factors may have played a role, such as self-selection bias
However, the researchers noted that self-selection bias does not explain the timing and scale of the observed drop in fertility.
 |
Moreover, birth rates in the Czech Republic dropped from 1.83 per 1,000 women in 2021 to 1.37 in 2024, adding further evidence that the COVID-19 vaccines may be contributing to the decline in fertility.

That downward trend, the researchers argue, supports the hypothesis that something beyond individual decision-making may be affecting conception rates.
As such, they argue that the study’s results warrant a closer and more thorough examination of the impact of mass vaccination.
 |
If this study holds true, and vaccinated women are really much less likely to have successful conceptions, the implications for humanity are massive.
 |
Millions of babies could be missing each year as a result of COVID vaccination, and recent data from Europe and beyond already point to a deeply disturbing trend.
NOTE: Europe experienced a sharper decline in births than usual from 2021 to 2023.
Live births fell from 4.09 million in 2021 to 3.67 million in 2023, marking a 10.3% decline in just two years.

The new Czech study adds to growing evidence that COVID vaccines may be contributing to a dramatic decline in fertility, just as many feared all along.
As Elon Musk warns, “If there are no humans, there’s no humanity.”
Whether the shots are the cause or not, the trend is real—and it’s accelerating.
It’s time to stop dismissing the signals and start investigating the cause.

Thanks for reading. I hope this report gave you real value. This is a critically important topic that deserves attention.
If you appreciate my work and want to help keep it going, consider becoming a paid subscriber.
99% of readers get this content for free. But just $5/month from the 1% keeps it flowing for everyone else.
If this work matters to you, this is the best way to support it.
Be the 1% who makes it possible.
Catch the rest of today’s biggest headlines at VigilantFox.com.
The Quiet Invasion: How Transnational Crime and Chinese State Actors Infiltrated Vancouver and Eroded Canada’s Sovereignty

RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued
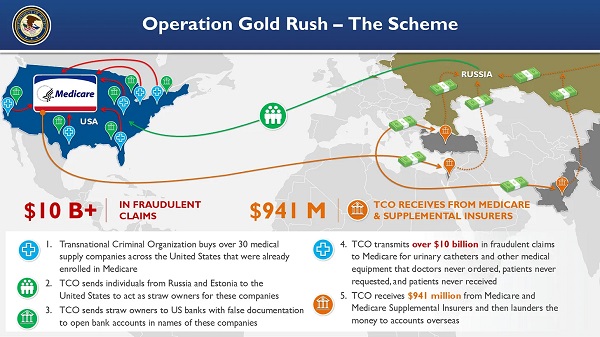
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
Business1 day ago
RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate
-
Crime2 days ago
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Business13 hours ago
Business13 hours agoWhy it’s time to repeal the oil tanker ban on B.C.’s north coast
-
 Censorship Industrial Complex1 day ago
Censorship Industrial Complex1 day agoGlobal media alliance colluded with foreign nations to crush free speech in America: House report
-
 Alberta7 hours ago
Alberta7 hours agoAlberta Provincial Police – New chief of Independent Agency Police Service
-
 Health2 days ago
Health2 days agoRFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
-
 Alberta12 hours ago
Alberta12 hours agoPierre Poilievre – Per Capita, Hardisty, Alberta Is the Most Important Little Town In Canada
-
 Business1 day ago
Business1 day agoElon Musk slams Trump’s ‘Big Beautiful Bill,’ calls for new political party