Brownstone Institute
The WHO’s Proposed Pandemic Agreements Worsen Public Health

From the Brownstone Institute
The WHO decided that the response for a Toronto aged care resident and a young mother in a Malawian village should be essentially the same – stop them from meeting family and working, then inject them with the same patented chemicals.
Much has been written on the current proposals putting the World Health Organization (WHO) front and center of future pandemic responses. With billions of dollars in careers, salaries, and research funding on the table, it is difficult for many to be objective. However, there are fundamentals here that everyone with public health training should agree upon. Most others, if they take time to consider, would also agree. Including, when divorced from party politicking and soundbites, most politicians.
So here, from an orthodox public health standpoint, are some problems with the proposals on pandemics to be voted on at the World Health Assembly at the end of this month.
Unfounded Messaging on Urgency
The Pandemic Agreement (treaty) and IHR amendments have been promoted based on claims of a rapidly increasing risk of pandemics. In fact, they pose an ‘existential threat’ (i.e. one that may end our existence) according to the G20’s High Level Independent Panel in 2022. However, the increase in reported natural outbreaks on which the WHO, the World Bank, G20, and others based these claims is shown to be unfounded in a recent analysis from the UK’s University of Leeds. The main database on which most outbreak analyses rely, the GIDEON database, shows a reduction in natural outbreaks and resultant mortality over the past 10 to 15 years, with the prior increase between 1960 and 2000 fully consistent with the development of the technologies necessary to detect and record such outbreaks; PCR, antigen and serology tests, and genetic sequencing.
The WHO does not refute this but simply ignores it. Nipah viruses, for example, only ‘emerged’ in the late 1990s when we found ways to actually detect them. Now we can readily distinguish new variants of coronavirus to promote uptake of pharmaceuticals. The risk does not change by detecting them; we just change the ability to notice them. We also have the ability to modify viruses to make them worse – this is a relatively new problem. But do we really want an organization influenced by China, with North Korea on its executive board (insert your favorite geopolitical rivals), to manage a future bioweapons emergency?
Irrespective of growing evidence that Covid-19 was not a natural phenomenon, modelling that the World Bank quotes as suggesting a 3x increase in outbreaks over the next decade actually predicts that a Covid-like event will recur less than once per century. Diseases that the WHO uses to suggest an increase in outbreaks over the past 20 years, including cholera, plague, yellow fever, and influenza variants were orders of magnitude worse in past centuries.
This all makes it doubly confusing that the WHO is breaking its own legal requirements in order to push through a vote without Member States having time to properly review implications of the proposals. The urgency must be for reasons other than public health need. Others can speculate why, but we are all human and all have egos to protect, even when preparing legally binding international agreements.
Low Relative Burden
The burden (e.g. death rate or life years lost) of acute outbreaks is a fraction of the overall disease burden, far lower than many endemic infectious diseases such as malaria, HIV, and tuberculosis, and a rising burden of non-communicable disease. Few natural outbreaks over the past 20 years have resulted in more than 1,000 deaths – or 8 hours of tuberculosis mortality. Higher-burden diseases should dominate public health priorities, however dull or unprofitable they may seem.
With the development of modern antibiotics, major outbreaks from the big scourges of the past like Plague and typhus ceased to occur. Though influenza is caused by a virus, most deaths are also due to secondary bacterial infections. Hence, we have not seen a repeat of the Spanish flu in over a century. We are better at healthcare than we used to be and have improved nutrition (generally) and sanitation. Widespread travel has eliminated the risks of large immunologically naive populations, making our species more immunologically resilient. Cancer and heart disease may be increasing, but infectious diseases overall are declining. So where should we focus?
Lack of Evidence Base
Investment in public health requires both evidence (or high likelihood) that the investment will improve outcomes and an absence of significant harm. The WHO has demonstrated neither with their proposed interventions. Neither has anyone else. The lockdown and mass vaccination strategy promoted for Covid-19 resulted in a disease that predominantly affects elderly sick people leading to 15 million excess deaths, even increasing mortality in young adults. In past acute respiratory outbreaks, things got better after one or perhaps two seasons, but with Covid-19 excess mortality persisted.
Within public health, this would normally mean we check whether the response caused the problem. Especially if it’s a new type of response, and if past understanding of disease management predicted that it would. This is more reliable than pretending that past knowledge did not exist. So again, the WHO (and other public-private partnerships) are not following orthodox public health, but something quite different.
Centralization for a Highly Heterogeneous Problem
Twenty-five years ago, before private investors became so interested in public health, it was accepted that decentralization was sensible. Providing local control to communities that could then prioritize and tailor health interventions themselves can provide better outcomes. Covid-19 underlined the importance of this, showing how uneven the impact of an outbreak is, determined by population age, density, health status, and many other factors. To paraphrase the WHO, ‘Most people are safe, even when some are not.’
However, for reasons that remain unclear to many, the WHO decided that the response for a Toronto aged care resident and a young mother in a Malawian village should be essentially the same – stop them from meeting family and working, then inject them with the same patented chemicals. The WHO’s private sponsors, and even the two largest donor countries with their strong pharmaceutical sectors, agreed with this approach. So too did the people paid to implement it. It was really only history, common sense, and public health ethics that stood in the way, and they proved much more malleable.
Absence of Prevention Strategies Through Host Resilience
The WHO IHR amendments and Pandemic Agreement are all about detection, lockdowns, and mass vaccination. This would be good if we had nothing else. Fortunately, we do. Sanitation, better nutrition, antibiotics, and better housing halted the great scourges of the past. An article in the journal Nature in 2023 suggested that just getting vitamin D at the right level may have cut Covid-19 mortality by a third. We already knew this and can speculate on why it became controversial. It’s really basic immunology.
Nonetheless, nowhere within the proposed US$30+ billion annual budget is any genuine community and individual resilience supported. Imagine putting a few billion more into nutrition and sanitation. Not only would you dramatically reduce mortality from occasional outbreaks, but more common infectious diseases, and metabolic diseases such as diabetes and obesity, would also go down. This would actually reduce the need for pharmaceuticals. Imagine a pharmaceutical company, or investor, promoting that. It would be great for public health, but a suicidal business approach.
Conflicts of Interest
All of which brings us, obviously, to conflicts of interest. The WHO, when formed, was essentially funded by countries through a core budget, to address high-burden diseases on country request. Now, with 80% of its use of funds specified directly by the funder, its approach is different. If that Malawian village could stump up tens of millions for a program, they would get what they ask for. But they don’t have that money; Western countries, Pharma, and software moguls do.
Most people on earth would grasp that concept far better than a public health workforce heavily incentivized to think otherwise. This is why the World Health Assembly exists and has the ability to steer the WHO in directions that don’t harm their populations. In its former incarnation, the WHO considered conflict of interest to be a bad thing. Now, it works with its private and corporate sponsors, within the limits set by its Member States, to mold the world to their liking.
The Question Before Member States
To summarize, while it’s sensible to prepare for outbreaks and pandemics, it’s even more sensible to improve health. This involves directing resources to where the problems are and using them in a way that does more good than harm. When people’s salaries and careers become dependent on changing reality, reality gets warped. The new pandemic proposals are very warped. They are a business strategy, not a public health strategy. It is the business of wealth concentration and colonialism – as old as humanity itself.
The only real question is whether the majority of the Member States of the World Health Assembly, in their voting later this month, wish to promote a lucrative but rather amoral business strategy, or the interests of their people.
Author


From the Brownstone Institute

Way back in the B.C. era (Before Covid), I taught Medical Humanities and Bioethics at an American medical school. One of my older colleagues – I’ll call him Dr. Quinlan – was a prominent member of the faculty and a nationally recognized proponent of physician-assisted suicide.
Dr. Quinlan was a very nice man. He was soft-spoken, friendly, and intelligent. He had originally become involved in the subject of physician-assisted suicide by accident, while trying to help a patient near the end of her life who was suffering terribly.
That particular clinical case, which Dr. Quinlan wrote up and published in a major medical journal, launched a second career of sorts for him, as he became a leading figure in the physician-assisted suicide movement. In fact, he was lead plaintiff in a challenge of New York’s then-prohibition against physician-assisted suicide.
The case eventually went all the way to the US Supreme Court, which added to his fame. As it happened, SCOTUS ruled 9-0 against him, definitively establishing that there is no “right to die” enshrined in the Constitution, and affirming that the state has a compelling interest to protect the vulnerable.
SCOTUS’s unanimous decision against Dr. Quinlan meant that his side had somehow pulled off the impressive feat of uniting Antonin Scalia, Ruth Bader Ginsberg, and all points in between against their cause. (I never quite saw how that added to his luster, but such is the Academy.)
At any rate, I once had a conversation with Dr. Quinlan about physician-assisted suicide. I told him that I opposed it ever becoming legal. I recall he calmly, pleasantly asked me why I felt that way.
First, I acknowledged that his formative case must have been very tough, and allowed that maybe, just maybe, he had done right in that exceptionally difficult situation. But as the legal saying goes, hard cases make bad law.
Second, as a clinical physician, I felt strongly that no patient should ever see their doctor and have to wonder if he was coming to help keep them alive or to kill them.
Finally, perhaps most importantly, there’s this thing called the slippery slope.
As I recall, he replied that he couldn’t imagine the slippery slope becoming a problem in a matter so profound as causing a patient’s death.
Well, maybe not with you personally, Dr. Quinlan, I thought. I said no more.
But having done my residency at a major liver transplant center in Boston, I had had more than enough experience with the rather slapdash ethics of the organ transplantation world. The opaque shuffling of patients up and down the transplant list, the endless and rather macabre scrounging for donors, and the nebulous, vaguely sinister concept of brain death had all unsettled me.
Prior to residency, I had attended medical school in Canada. In those days, the McGill University Faculty of Medicine was still almost Victorian in its ways: an old-school, stiff-upper-lip, Workaholics-Anonymous-chapter-house sort of place. The ethic was hard work, personal accountability for mistakes, and above all primum non nocere – first, do no harm.
Fast forward to today’s soft-core totalitarian state of Canada, the land of debanking and convicting peaceful protesters, persecuting honest physicians for speaking obvious truth, fining people $25,000 for hiking on their own property, and spitefully seeking to slaughter harmless animals precisely because they may hold unique medical and scientific value.
To all those offenses against liberty, morality, and basic decency, we must add Canada’s aggressive policy of legalizing, and, in fact, encouraging industrial-scale physician-assisted suicide. Under Canada’s Medical Assistance In Dying (MAiD) program, which has been in place only since 2016, physician-assisted suicide now accounts for a terrifying 4.7 percent of all deaths in Canada.
MAiD will be permitted for patients suffering from mental illness in Canada in 2027, putting it on par with the Netherlands, Belgium, and Switzerland.
To its credit, and unlike the Netherlands and Belgium, Canada does not allow minors to access MAiD. Not yet.
However, patients scheduled to be terminated via MAiD in Canada are actively recruited to have their organs harvested. In fact, MAiD accounts for 6 percent of all deceased organ donors in Canada.
In summary, in Canada, in less than 10 years, physician-assisted suicide has gone from illegal to both an epidemic cause of death and a highly successful organ-harvesting source for the organ transplantation industry.
Physician-assisted suicide has not slid down the slippery slope in Canada. It has thrown itself off the face of El Capitan.
And now, at long last, physician-assisted suicide may be coming to New York. It has passed the House and Senate, and just awaits the Governor’s signature. It seems that the 9-0 Supreme Court shellacking back in the day was just a bump in the road. The long march through the institutions, indeed.
For a brief period in Western history, roughly from the introduction of antibiotics until Covid, hospitals ceased to be a place one entered fully expecting to die. It appears that era is coming to an end.
Covid demonstrated that Western allopathic medicine has a dark, sadistic, anti-human side – fueled by 20th-century scientism and 21st-century technocratic globalism – to which it is increasingly turning. Physician-assisted suicide is a growing part of this death cult transformation. It should be fought at every step.
I have not seen Dr. Quinlan in years. I do not know how he might feel about my slippery slope argument today.
I still believe I was correct.
From the Brownstone Institute

Many news outlets reported the announcement of the Nobel Peace Prize on Friday by saying President Donald Trump had missed out (Washington Post, Yahoo, Hindustan Times, Huffington Post), not won (USA Today), fallen short (AP News), lost (Time), etc. There is even a meme doing the rounds about ‘Trump Wine.’ ‘Made from sour grapes,’ the label explains, ‘This is a full bodied and bitter vintage guaranteed to leave a nasty taste in your mouth for years.’

For the record, the prize was awarded to María Corina Machado for her courageous and sustained opposition to Venezuela’s ruling regime. Trump called to congratulate her. Given his own attacks on the Venezuelan president, his anger will be partly mollified, and he could even back her with practical support. He nonetheless attacked the prize committee, and the White House assailed it for putting politics before peace.
He could be in serious contention next year. If his Gaza peace plan is implemented and holds until next October, he should get it. That he is unlikely to do so is more a reflection on the award and less on Trump.
So He Won the Nobel Peace Prize. Meh!
Alfred Nobel’s will stipulates the prize should be awarded to the person who has contributed the most to promote ‘fraternity between nations…abolition or reduction of standing armies and…holding and promotion of peace congresses.’ Over the decades, this has expanded progressively to embrace human rights, political dissent, environmentalism, race, gender, and other social justice causes.
On these grounds, I would have thought the Covid resistance should have been a winner. The emphasis has shifted from outcomes and actual work to advocacy. In honouring President Barack Obama in 2009, the Nobel committee embarrassed itself, patronised him, and demeaned the prize. His biggest accomplishment was the choice of his predecessor as president: the prize was a one-finger send-off to President George W. Bush.
There have been other strange laureates, including those prone to wage war (Henry Kissinger, 1973), tainted through association with terrorism (Yasser Arafat, 1994), and contributions to fields beyond peace, such as planting millions of trees. Some laureates were subsequently discovered to have embellished their record, and others proved to be flawed champions of human rights who had won them the treasured accolade.
Conversely, Mahatma Gandhi did not get the prize, not for his contributions to the theory and practice of non-violence, nor for his role in toppling the British Raj as the curtain raiser to worldwide decolonisation. The sad reality is how little practical difference the prize has made to the causes it espoused. They bring baubles and honour to the laureates, but the prize has lost much of its lustre as far as results go.
Trump Was Not a Serious Contender
The nomination processes start in September and nominations close on 31 January. The five-member Norwegian Nobel committee scrutinises the list of candidates and whittles it down between February and October. The prize is announced on or close to 10 October, the date Alfred Nobel died, and the award ceremony is held in Oslo in early December.
The calendar rules out a newly elected president in his first year, with the risible exception of Obama. The period under review was 2024. Trump’s claims to have ended seven wars and boasts of ‘nobody’s ever done that’ are not taken seriously beyond the narrow circle of fervent devotees, sycophantic courtiers, and supplicant foreign leaders eager to ingratiate themselves with over-the-top flattery.
Trump Could Be in Serious Contention Next Year
Trump’s 20-point Gaza peace plan falls into three conceptual-cum-chronological parts: today, tomorrow, and the day after. At the time of writing, in a hinge moment in the two-year war, Israel has implemented a ceasefire in Gaza, Hamas has agreed to release Israeli hostages on 13-14 October, and Israel will release around 2,000 Palestinian prisoners (today’s agenda). So why are the ‘Ceasefire Now!’ mobs not out on the streets celebrating joyously instead of looking morose and discombobulated? Perhaps they’ve been robbed of the meaning of life?
The second part (tomorrow) requires Hamas demilitarisation, surrender, amnesty, no role in Gaza’s future governance, resumption of aid deliveries, Israeli military pullbacks, a temporary international stabilisation force, and a technocratic transitional administration. The third part, the agenda for the day after, calls for the deradicalisation of Gaza, its reconstruction and development, an international Peace Board to oversee implementation of the plan, governance reforms of the Palestinian Authority, and, over the horizon, Palestinian statehood.
There are too many potential pitfalls to rest easy on the prospects for success. Will Hamas commit military and political suicide? How can the call for democracy in Gaza and the West Bank be reconciled with Hamas as the most popular group among Palestinians? Can Israel’s fractious governing coalition survive?
Both Hamas and Israel have a long record of agreeing to demands under pressure but sabotaging their implementation at points of vulnerability. The broad Arab support could weaken as difficulties arise. The presence of the internationally toxic Tony Blair on the Peace Board could derail the project. Hamas has reportedly called on all factions to reject Blair’s involvement. Hamas official Basem Naim, while thanking Trump for his positive role in the peace deal, explained that ‘Palestinians, Arabs and Muslims and maybe a lot [of] people around the world still remember his [Blair’s] role in causing the killing of thousands or millions of innocent civilians in Afghanistan and Iraq.’
It would be a stupendous achievement for all the complicated moving parts to come together in stable equilibrium. What cannot and should not be denied is the breathtaking diplomatic coup already achieved. Only Trump could have pulled this off.
The very traits that are so offputting in one context helped him to get here: narcissism; bullying and impatience; bull in a china shop style of diplomacy; indifference to what others think; dislike of wars and love of real estate development; bottomless faith in his own vision, negotiating skills, and ability to read others; personal relationships with key players in the region; and credibility as both the ultimate guarantor of Israel’s security and preparedness to use force if obstructed. Israelis trust him; Hamas and Iran fear him.
The combined Israeli-US attacks to degrade Iran’s nuclear capability underlined the credibility of threats of force against recalcitrant opponents. Unilateral Israeli strikes on Hamas leaders in Qatar highlighted to uninvolved Arabs the very real dangers of continued escalation amidst the grim Israeli determination to rid themselves of Hamas once and for all.
Trump Is Likely to Be Overlooked
Russia has sometimes been the object of the Nobel Peace Prize. The mischievous President Vladimir Putin has suggested Trump may be too good for the prize. Trump’s disdain for and hostility to international institutions and assaults on the pillars of the liberal international order would have rubbed Norwegians, among the world’s strongest supporters of rules-based international governance, net zero, and foreign aid, the wrong way.
Brash and public lobbying for the prize, like calling the Norwegian prime minister, is counterproductive. The committee is fiercely independent. Nominees are advised against making the nomination public, let alone orchestrating an advocacy campaign. Yet, one laureate is believed to have mobilised his entire government for quiet lobbying behind the scenes, and another to have bad-mouthed a leading rival to friendly journalists.
Most crucially, given that Scandinavian character traits tip towards the opposite end of the scale, it’s hard to see the committee overlooking Trump’s loud flaws, vanity, braggadocio, and lack of grace and humility. Trump supporters discount his character traits and take his policies and results seriously. Haters cannot get over the flaws to seriously evaluate policies and outcomes. No prizes for guessing which group the Nobel committee is likely to belong to. As is currently fashionable to say when cancelling someone, Trump’s values do not align with those of the committee and the ideals of the prize.
Author



Parliament Forces Liberals to Release Stellantis Contracts After $15-Billion Gamble Blows Up In Taxpayer Faces

US government buys stakes in two Canadian mining companies

Plan Ahead: Voting May Take a Little Longer This Election Day
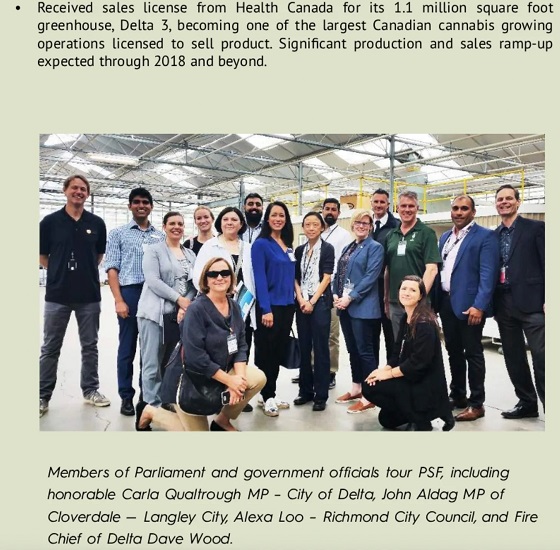
Politically Connected Canadian Weed Sellers Push Back in B.C. Court, Seek Distance from Convicted Heroin Trafficker
-
 Business1 day ago
Business1 day ago$15B and No Guarantees? Stellantis Deal explained by former Conservative Shadow Minister of Innovation, Science and Technology
-
 Alberta22 hours ago
Alberta22 hours agoPremier Smith moves to protect Alberta in International Agreements
-
 Business18 hours ago
Business18 hours agoLiberals backtrack on bill banning large cash gifts, allowing police to search Canadians’ mail
-
 Agriculture1 day ago
Agriculture1 day agoFrom Underdog to Top Broodmare
-
 Health17 hours ago
Health17 hours agoFor Anyone Planning on Getting or Mandating Others to Get an Influenza Vaccine (Flu Shot)
-
 Sports17 hours ago
Sports17 hours ago‘We Follow The Money’: Kash Patel Says Alleged NBA Ties To Mafia Just ‘The Start’ Of FBI Investigation
-
 Alberta2 days ago
Alberta2 days agoAlberta’s licence plate vote is down to four
-
 Bruce Dowbiggin2 days ago
Bruce Dowbiggin2 days agoIs The Latest Tiger Woods’ Injury Also A Death Knell For PGA Champions Golf?