Addictions
Reckless: British Columbia’s “safe supply” fentanyl tablet experiment
From the MacDonald Laurier Institute
By Adam Zivo
While safer supply sounds nice in theory, addiction experts have found that drug users are reselling (“diverting”) a significant portion of their free hydromorphone on the black market to purchase harder substances. This has fuelled new addictions while generating handsome profits for organized crime.
Adam Zivo reviews the latest drug protocols adopted by the BC government and reports on their alarming lack of evidence and accountability.
British Columbia’s new drug protocols allow doctors throughout the province to prescribe “safer supply” drugs in a reckless manner.
In a new report titled Reckless: British Columbia’s “safe supply” fentanyl tablet experiment, Adam Zivo reviews the newest drug protocols adopted by the BC government, documenting the evolution of “safe supply” opioid programs in Canada since 2020. Zivo reports on the concerning lack of evidence behind the protocols, how they undermine recovery, drive diversion to the black market, and ruin the lives of young Canadians.
The new protocols not only avoid any requirement for drug users to first try evidence-based recovery programs before receiving high-potency opioids, but also allow minors to receive them, with no reference to the rights and roles of parents or even a minimum age for safer supply clients.
Of deep concern is also the BC government’s approach of continually increasing access to “safe” opioids despite openly admitting that there is no evidence of proven benefits or safety. The protocols also require that clients be told that their access to free fentanyl and sufentanil will almost certainly be cut off if they are hospitalized, or if they attend withdrawal management or substance use treatment facilities.
Zivo explains: “The prospect of free fentanyl and sufentanil creates powerful incentives to sign away one’s rights to evidence based treatment, so the province is essentially exploiting clients’ addictions so that it can experiment on them without taking legal responsibility for potential harms.”
Zivo adds that “one can reasonably expect that a significant portion of the fentanyl tablets being distributed by the BC government will end up being traded or resold on the black market,” explaining how mass diversion is already a major issue for weaker “safer supply” opioids like hydromorphone.
While addiction experts have been overwhelmingly critical of unsupervised safer supply, Zivo notes that many believe that the solution is not to abolish but to reform the program so that drugs can be provided more responsibly. By receiving safer supply as a temporary intervention, addicted users can transition to recovery-oriented treatments such as opioid agonist therapy (OAT.)
“It would not take much to reshape BC’s safer supply fentanyl and sufentanil programs into something more responsible and genuinely safe,” concludes Zivo. “There is nothing preventing the province from redesigning safer supply as a recovery-oriented intervention.”
To learn more, read the full paper here:


Executive Summary
This past August, British Columbia’s government quietly launched new protocols that allow doctors to prescribe “safer supply” fentanyl tablets and liquid sufentanil. Fentanyl is at least 10 times stronger than hydromorphone and sufentanil, which is derived from fentanyl, is a further 5 to 10 times more potent than its parent drug. While in theory these drugs could save lives if provisioned cautiously, the way the province has chosen to distribute these dangerous opioids is nothing short of reckless.
There is evidence to support the use of opioid agonist therapy (“OAT”) medications, such as methadone, buprenorphine, and slow release oral morphine in addiction treatment, but the government’s new protocols extrapolate OAT-related evidence to support “safer supply” fentanyl even though the two therapies have little in common. In fact, the government’s protocols stress that providing safer supply fentanyl or sufentanil is “not a treatment for opioid use disorder” and that “there is no evidence available supporting this intervention, safety data, or established best practices for when and how to provide it.” It is deeply concerning that the BC government has, over the past several years, significantly increased access to “safe” fentanyl and sufentanil despite openly admitting that there is no evidence showing that these interventions provide any benefits and can be implemented safely.
“Safer supply” programs claim to reduce overdoses and deaths by providing free pharmaceutical-grade drugs as alternatives to potentially tainted illicit substances. While safer supply sounds nice in theory, addiction experts have found that drug users are reselling (“diverting”) a significant portion of their free hydromorphone on the black market to purchase harder substances. This has fuelled new addictions while generating handsome profits for organized crime. Some patients have even been coerced into securing safer supply they didn’t need. Pimps and abusive partners pressure vulnerable women into securing as much hydromorphone as possible for black market resale. Other vulnerable patients, such as the geriatric and disabled, have been robbed of their safer supply outside of pharmacies.
There are other issues with the protocols, too. They require that clients be told that their access to free fentanyl and sufentanil will almost certainly be cut off if they are hospitalized, or if they attend withdrawal management or substance use treatment facilities. This creates powerful disincentives for drug users to seek life-saving health care. Further, none of the safer supply protocols by the British Columbia Centre on Substance Use (BCCSU) discuss the rights and roles of the parents of minors struggling with addiction. It appears that health care providers can give fentanyl and sufentanil to minors regardless of whether parents are aware of, or consent to, this intervention. The protocols do not specify a minimum age for safer supply clients.
It would not take much to reshape BC’s safer supply fentanyl and sufentanil programs into something more responsible and genuinely safe. There is nothing preventing the province from redesigning safer supply as a recovery-oriented intervention. Experts argue that safer supply could be helpful if used as a temporary intervention that helps severely-addicted users make the transition to recovery-oriented treatments, such as OAT.
There is also nothing stopping the province from fixing many of the issues with the safer supply program – including lax safeguards for youth. Any safer supply model must require supervised consumption. It is the absence of this supervision that has enabled the mass diversion of safer supply drugs onto the black market.
Governments have a duty to provide evidence-based treatment to vulnerable citizens and consider collateral harms to others. Rather than fulfil this duty, the BC government is committing to risky and highly experimental interventions that lack an appropriate evidence base.
Adam Zivo is a freelance writer and political analyst best known for his weekly columns in the National Post. He holds a Master of Public Policy from the Munk School of Global Affairs and Public Policy and recently founded the Centre for Responsible Drug Policy, a nonprofit advocacy organization.

2025 Federal Election
Poilievre to invest in recovery, cut off federal funding for opioids and defund drug dens

From Conservative Party Communications
Poilievre will Make Recovery a Reality for 50,000 Canadians
Conservative Leader Pierre Poilievre pledged he will bring the hope that our vulnerable Canadians need by expanding drug recovery programs, creating 50,000 new opportunities for Canadians seeking freedom from addiction. At the same time, he will stop federal funding for opioids, defund federal drug dens, and ensure that any remaining sites do not operate within 500 meters of schools, daycares, playgrounds, parks and seniors’ homes, and comply with strict new oversight rules that focus on pathways to treatment.
More than 50,000 people have lost their lives to fentanyl since 2015—more Canadians than died in the Second World War. Poilievre pledged to open a path to recovery while cracking down on the radical Liberal experiment with free access to illegal drugs that has made the crisis worse and brought disorder to local communities.
Specifically, Poilievre will:
- Fund treatment for 50,000 Canadians. A new Conservative government will fund treatment for 50,000 Canadians in treatment centres with a proven record of success at getting people off drugs. This includes successful models like the Bruce Oake Recovery Centre, which helps people recover and reunite with their families, communities, and culture. To ensure the best outcomes, funding will follow results. Where spaces in good treatment programs exist, we will use them, and where they need to expand, these funds will allow that.
- Ban drug dens from being located within 500 metres of schools, daycares, playgrounds, parks, and seniors’ homes and impose strict new oversight rules. Poilievre also pledged to crack down on the Liberals’ reckless experiments with free access to illegal drugs that allow provinces to operate drug sites with no oversight, while pausing any new federal exemptions until evidence justifies they support recovery. Existing federal sites will be required to operate away from residential communities and places where families and children frequent and will now also have to focus on connecting users with treatment, meet stricter regulatory standards or be shut down. He will also end the exemption for fly-by-night provincially-regulated sites.
“After the Lost Liberal Decade, Canada’s addiction crisis has spiralled out of control,” said Poilievre. “Families have been torn apart while children have to witness open drug use and walk through dangerous encampments to get to school. Canadians deserve better than the endless Liberal cycle of crime, despair, and death.”
Since the Liberals were first elected in 2015, our once-safe communities have become sordid and disordered, while more and more Canadians have been lost to the dangerous drugs the Liberals have flooded into our streets. In British Columbia, where the Liberals decriminalized dangerous drugs like fentanyl and meth, drug overdose deaths increased by 200 percent.
The Liberals also pursued a radical experiment of taxpayer-funded hard drugs, which are often diverted and resold to children and other vulnerable Canadians. The Vancouver Police Department has said that roughly half of all hydromorphone seizures were diverted from this hard drugs program, while the Waterloo Regional Police Service and Niagara Regional Police Service said that hydromorphone seizures had exploded by 1,090% and 1,577%, respectively.
Despite the death and despair that is now common on our streets, bizarrely Mark Carney told a room of Liberal supporters that 50,000 fentanyl deaths in Canada is not “a crisis.” He also hand-picked a Liberal candidate who said the Liberals “would be smart to lean into drug decriminalization” and another who said “legalizing all drugs would be good for Canada.”
Carney’s star candidate Gregor Robertson, an early advocate of decriminalization and so-called safe supply, wanted drug dens imposed on communities without any consultation or public safety considerations. During his disastrous tenure as Vancouver Mayor, overdoses increased by 600%.
Alberta has pioneered an approach that offers real hope by adopting a recovery-focused model of care, leading to a nearly 40 percent reduction in drug-poisoning deaths since 2023—three times the decrease seen in British Columbia. However, we must also end the Liberal drug policies that have worsened the crisis and harmed countless lives and families.
To fund this policy, a Conservative government will stop federal funding for opioids, defund federal drug dens, and sue the opioid manufacturers and consulting companies who created this crisis in the first place.
“Canadians deserve better than the Liberal cycle of crime, despair, and death,” said Poilievre. “We will treat addiction with compassion and accountability—not with more taxpayer-funded poison. We will turn hurt into hope by shutting down drug dens, restoring order in our communities, funding real recovery, and bringing our loved ones home drug-free.”


By Adam Zivo
Sweden, the U.K., and Canada all experimented with providing opioids to addicts. The results were disastrous.
[This article was originally published in City Journal, a public policy magazine and website published by the Manhattan Institute for Policy Research. We encourage our readers to subscribe to them for high-quality analysis on urban issues]
Last August, Denver’s city council passed a proclamation endorsing radical “harm reduction” strategies to address the drug crisis. Among these was “safer supply,” the idea that the government should give drug users their drug of choice, for free. Safer supply is a popular idea among drug-reform activists. But other countries have already tested this experiment and seen disastrous results, including more addiction, crime, and overdose deaths. It would be foolish to follow their example.
The safer-supply movement maintains that drug-related overdoses, infections, and deaths are driven by the unpredictability of the black market, where drugs are inconsistently dosed and often adulterated with other toxic substances. With ultra-potent opioids like fentanyl, even minor dosing errors can prove fatal. Drug contaminants, which dealers use to provide a stronger high at a lower cost, can be just as deadly and potentially disfiguring.
Because of this, harm-reduction activists sometimes argue that governments should provide a free supply of unadulterated, “safe” drugs to get users to abandon the dangerous street supply. Or they say that such drugs should be sold in a controlled manner, like alcohol or cannabis—an endorsement of partial or total drug legalization.
But “safe” is a relative term: the drugs championed by these activists include pharmaceutical-grade fentanyl, hydromorphone (an opioid as potent as heroin), and prescription meth. Though less risky than their illicit alternatives, these drugs are still profoundly dangerous.
The theory behind safer supply is not entirely unreasonable, but in every country that has tried it, implementation has led to increased suffering and addiction. In Europe, only Sweden and the U.K. have tested safer supply, both in the 1960s. The Swedish model gave more than 100 addicts nearly unlimited access through their doctors to prescriptions for morphine and amphetamines, with no expectations of supervised consumption. Recipients mostly sold their free drugs on the black market, often through a network of “satellite patients” (addicts who purchased prescribed drugs). This led to an explosion of addiction and public disorder.
Most doctors quickly abandoned the experiment, and it was shut down after just two years and several high-profile overdose deaths, including that of a 17-year-old girl. Media coverage portrayed safer supply as a generational medical scandal and noted that the British, after experiencing similar problems, also abandoned their experiment.
While the U.S. has never formally adopted a safer-supply policy, it experienced something functionally similar during the OxyContin crisis of the 2000s. At the time, access to the powerful opioid was virtually unrestricted in many parts of North America. Addicts turned to pharmacies for an easy fix and often sold or traded their extra pills for a quick buck. Unscrupulous “pill mills” handed out prescriptions like candy, flooding communities with OxyContin and similar narcotics. The result was a devastating opioid epidemic—one that rages to this day, at a cumulative cost of hundreds of thousands of American lives. Canada was similarly affected.
The OxyContin crisis explains why many experienced addiction experts were aghast when Canada greatly expanded access to safer supply in 2020, following a four-year pilot project. They worried that the mistakes of the recent past were being made all over again, and that the recently vanquished pill mills had returned under the cloak of “harm reduction.”
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Most Canadian safer-supply prescribers dispense large quantities of hydromorphone with little to no supervised consumption. Patients can receive up to 40 eight-milligram pills per day—despite the fact that just two or three are enough to cause an overdose in someone without opioid tolerance. Some prescribers also provide supplementary fentanyl, oxycodone, or stimulants.
Unfortunately, many safer-supply patients sell or trade a significant portion of these drugs—primarily hydromorphone—in order to purchase more potent illicit substances, such as street fentanyl.
The problems with safer supply entered Canada’s consciousness in mid-2023, through an investigative report I wrote for the National Post. I interviewed 14 addiction physicians from across the country, who testified that safer-supply diversion is ubiquitous; that the street price of hydromorphone collapsed by up to 95 percent in communities where safer supply is available; that youth are consuming and becoming addicted to diverted safer-supply drugs; and that organized crime traffics these drugs.
Facing pushback, I interviewed former drug users, who estimated that roughly 80 percent of the safer-supply drugs flowing through their social circles was getting diverted. I documented dozens of examples of safer-supply trafficking online, representing tens of thousands of pills. I spoke with youth who had developed addictions from diverted safer supply and adults who had purchased thousands of such pills.
After months of public queries, the police department of London, Ontario—where safer supply was first piloted—revealed last summer that annual hydromorphone seizures rose over 3,000 percent between 2019 and 2023. The department later held a press conference warning that gangs clearly traffic safer supply. The police departments of two nearby midsize cities also saw their post-2019 hydromorphone seizures increase more than 1,000 percent.
The Canadian government quietly dropped its support for safer supply last year, cutting funding for many of its pilot programs. The province of British Columbia (the nexus of the harm-reduction movement) finally pulled back support last month, after a leaked presentation confirmed that safer-supply drugs are getting sold internationally and that the government is investigating 60 pharmacies for paying kickbacks to safer-supply patients. For now, all safer-supply drugs dispensed within the province must be consumed under supervision.
Harm-reduction activists have insisted that no hard evidence exists of widespread diversion of safer-supply drugs, but this is only because they refuse to study the issue. Most “studies” supporting safer supply are produced by ideologically driven activist-scholars, who tend to interview a small number of program enrollees. These activists also reject attempts to track diversion as “stigmatizing.”
The experiences of Sweden, the United Kingdom, and Canada offer a clear warning: safer supply is a reliably harmful policy. The outcomes speak for themselves—rising addiction, diversion, and little evidence of long-term benefit.
As the debate unfolds in the United States, policymakers would do well to learn from these failures. Americans should not be made to endure the consequences of a policy already discredited abroad simply because progressive leaders choose to ignore the record. The question now is whether we will repeat others’ mistakes—or chart a more responsible course.
Our content is always free –
but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.


RCMP memo warns of Chinese interference on Canadian university campuses to affect election

WATCH: Massive Crowd for Historic Edmonton Poilievre Rally
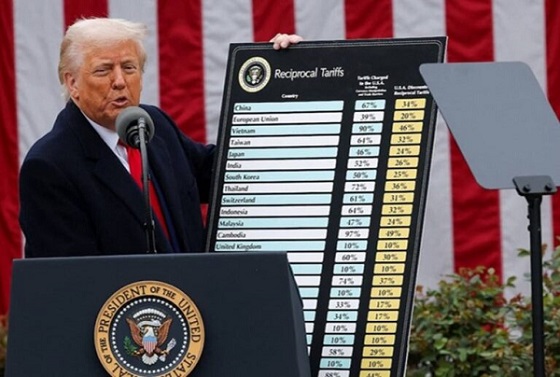
Trump threatens additional 50% tariffs on China, urges ‘patience’

Conservative Party urges investigation into Carney plan to spend $1 billion on heat pumps
-
2025 Federal Election1 day ago
RCMP memo warns of Chinese interference on Canadian university campuses to affect election
-
 Alberta2 days ago
Alberta2 days agoAlberta takes big step towards shorter wait times and higher quality health care
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoResearchers Link China’s Intelligence and Elite Influence Arms to B.C. Government, Liberal Party, and Trudeau-Appointed Senator
-
 Business2 days ago
Business2 days agoTrump raises China tariffs to 125%, announces 90-day pause for countries who’ve reached out to negotiate
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoThe status quo in Canadian politics isn’t sustainable for national unity
-
 Business1 day ago
Business1 day agoScott Bessent Says Trump’s Goal Was Always To Get Trading Partners To Table After Major Pause Announcement
-
 2025 Federal Election22 hours ago
2025 Federal Election22 hours agoTwo Canadian police unions endorse Pierre Poilievre for PM
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoPoilievre Announces Plan To Cut Taxes By $100,000 Per Home