Addictions
Province expanding recovery support in Red Deer
In Red Deer, Alberta’s government is increasing access to recovery-oriented care by launching several new initiatives within the community.
Alberta’s government has built a system of care based on the belief that recovery is possible for those suffering from the disease of addiction. The focus has been on reducing barriers to recovery by increasing capacity and ensuring that no one is forced to pay for life-saving addiction treatment. Since 2019, the province has added more than 10,000 new addiction treatment spaces. It has also removed financial barriers and pioneered a program for immediate, same-day access to life-saving evidence-based treatment medication.
Red Deer is home to Alberta’s first of 11 recovery communities being built by the province. This facility opened its doors in May 2023 and has become a beacon of hope for those suffering from addiction, along with their families. Red Deer was also the first in Alberta to open a Therapeutic Living Unit within its correctional center. This means the recovery community model of treatment has been adopted in corrections, lowering the chances of reoffending and breaking the cycle of addiction and crime in individuals’ lives. Access to opioid agonist therapy has been expanded to police cells through the Virtual Opioid Dependency Program and can also be administered by specialized paramedics with support from the province.
Earlier this year, Red Deer city council put forward and passed a motion requesting a transition of the drug consumption site to instead implement options focused on health, wellness and recovery.
In response to this request, Alberta’s government has committed $3.4 million to provide the following:
- A Mobile Rapid Access Addiction Medicine clinic operated by Recovery Alberta, located in the homeless shelter parking lot. This will offer screening, diagnosis and referral to services; access to the Virtual Opioid Dependency Program; and education, naloxone kits and needle exchange.
- A Dynamic Overdose Response Team of paramedics and licensed practical nurses to monitor a designated area of the Safe Harbour shelter facility, as well as the surrounding block.
- Recovery coaches in and around the homeless shelter to provide outreach services and help guide individuals along the path of recovery.
- Enhancements to medically supported detox capacity in partnership with Safe Harbour that will help more people safely withdraw from substances so they can continue their pursuit of recovery.
In addition, Alberta’s government recently provided more than $1.2 million over the next two years to the Red Deer Dream Centre to support 20 additional publicly funded addiction treatment beds.
“Our government will always listen to and take seriously the feedback we receive from elected local leaders. This is a well-thought-out plan that aligns with Red Deer’s needs and requests, which is why the province is making these changes and increasing support for the community. We remain committed to protecting the health and well-being of Albertans while actively supporting connections to treatment and recovery.”
“Our council is pleased to see this new path forward for recovery-oriented services in Red Deer. At the heart of our council’s and community’s efforts is the belief that recovery is possible for everyone, especially the most vulnerable. This is a complex challenge and only by working with all our partners at the province, agencies, businesses, faith communities and all Red Deerians will we create a safe, healthy and prosperous community. We look forward to close collaboration with the province as these changes are made.”
Alberta’s government is working closely with the City of Red Deer, Safe Harbour Society, Recovery Alberta and others to implement these supports starting this fall.
Since October 2018, the Red Deer drug consumption site has been operating at a temporary site within an ATCO trailer in the parking lot next to Safe Harbour Society’s detox building. As requested by the city council, the drug consumption site will be transitioned out of Red Deer once all other services are operational, which is anticipated to be in spring 2025. The program expansion for recovery services represents a net increase in programming and staffing.
“We look forward to bringing a new service to Red Deer with the opening of a Mobile Rapid Access Addiction Medicine clinic. With this and the new outreach services being put in place, Recovery Alberta will provide opportunities for those facing addiction and mental health issues to access support on an ongoing basis.”
“I am pleased to see that Alberta’s government is working collaboratively with our local government and service providers. This plan ensures we prioritize Red Deer’s needs while also supporting individuals in their pursuit of recovery.”
“Red Deer is a beautiful community with wonderful families and individuals. Transitioning the drug site out of Red Deer and focusing on recovery is the right thing to do. Thank you to the Government of Alberta and Red Deer City Council for leading, listening and doing what is right.”
“We are pleased to partner with Alberta’s government, Recovery Alberta and the City of Red Deer to increase access to addiction and detox services for those accessing supports at Safe Harbour. This partnership profoundly enhances our capacity to meet the needs of community members challenged by addiction and to support them in their recovery journey.”
Alberta is making record investments and removing barriers to recovery-oriented supports for all Albertans, regardless of where they live or their financial situation. This includes the addition of more than 10,000 new publicly funded addiction treatment spaces, expanded access to the Virtual Opioid Dependency Program—which provides same-day access to life-saving treatment medication—the removal of daily user fees for publicly funded live-in treatment, and the construction of 11 world-class recovery communities.
Quick facts
- Albertans struggling with opioid addiction can contact the Virtual Opioid Dependency Program (VODP) by calling 1-844-383-7688, seven days a week, from 6 a.m. to midnight. VODP provides same-day access to addiction medicine specialists. There is no wait list.
Related information
Related news


By Alexandra Keeler
The move follows explosive revelations that more than 60 B.C. pharmacies were allegedly participating in a scheme to overbill the government under its safer supply program. The scheme involved pharmacies incentivizing clients to fill prescriptions they did not require by offering them cash or rewards. Some of those clients then sold the drugs on the black market.
An addiction medicine advocacy group is urging B.C. to promptly issue new guidelines for witnessed dosing of drugs dispensed under the province’s controversial safer supply program.
In a March 24 letter to B.C.’s health minister, Addiction Medicine Canada criticized the BC Centre on Substance Use for dragging its feet on delivering the guidelines and downplaying the harms of prescription opioids.
The centre, a government-funded research hub, was tasked by the B.C. government with developing the guidelines after B.C. pledged in February to return to witnessed dosing. The government’s promise followed revelations that many B.C. pharmacies were exploiting rules permitting patients to take safer supply opioids home with them, leading to abuse of the program.
“I think this is just a delay,” said Dr. Jenny Melamed, a Surrey-based family physician and addiction specialist who signed the Addiction Medicine Canada letter. But she urged the centre to act promptly to release new guidelines.
“We’re doing harm and we cannot just leave people where they are.”
Addiction Medicine Canada’s letter also includes recommendations for moving clients off addictive opioids altogether.
“We should go back to evidence-based medicine, where we have medications that work for people in addiction,” said Melamed.
‘Best for patients’
On Feb. 19, the B.C. government said it would return to a witnessed dosing model. This model — which had been in place prior to the pandemic — will require safer supply participants to take prescribed opioids under the supervision of health-care professionals.
The move follows explosive revelations that more than 60 B.C. pharmacies were allegedly participating in a scheme to overbill the government under its safer supply program. The scheme involved pharmacies incentivizing clients to fill prescriptions they did not require by offering them cash or rewards. Some of those clients then sold the drugs on the black market.
In its Feb. 19 announcement, the province said new participants in the safer supply program would immediately be subject to the witnessed dosing requirement. For existing clients of the program, new guidelines would be forthcoming.
“The Ministry will work with the BC Centre on Substance Use to rapidly develop clinical guidelines to support prescribers that also takes into account what’s best for patients and their safety,” Kendra Wong, a spokesperson for B.C.’s health ministry, told Canadian Affairs in an emailed statement on Feb. 27.
More than a month later, addiction specialists are still waiting.
According to Addiction Medicine Canada’s letter, the BC Centre on Substance Use posed “fundamental questions” to the B.C. government, potentially causing the delay.
“We’re stuck in a place where the government publicly has said it’s told BCCSU to make guidance, and BCCSU has said it’s waiting for government to tell them what to do,” Melamed told Canadian Affairs.
This lag has frustrated addiction specialists, who argue the lack of clear guidance is impeding the transition to witnessed dosing and jeopardizing patient care. They warn that permitting take-home drugs leads to more diversion onto the streets, putting individuals at greater risk.
“Diversion of prescribed alternatives expands the number of people using opioids, and dying from hydromorphone and fentanyl use,” reads the letter, which was also co-signed by Dr. Robert Cooper and Dr. Michael Lester. The doctors are founding board members of Addiction Medicine Canada, a nonprofit that advises on addiction medicine and advocates for research-based treatment options.
“We have had people come in [to our clinic] and say they’ve accessed hydromorphone on the street and now they would like us to continue [prescribing] it,” Melamed told Canadian Affairs.
A spokesperson for the BC Centre on Substance Use declined to comment, referring Canadian Affairs to the Ministry of Health. The ministry was unable to provide comment by the publication deadline.
Big challenges
Under the witnessed dosing model, doctors, nurses and pharmacists will oversee consumption of opioids such as hydromorphone, methadone and morphine in clinics or pharmacies.
The shift back to witnessed dosing will place significant demands on pharmacists and patients. In April 2024, an estimated 4,400 people participated in B.C.’s safer supply program.
Chris Chiew, vice president of pharmacy and health-care innovation at the pharmacy chain London Drugs, told Canadian Affairs that the chain’s pharmacists will supervise consumption in semi-private booths.
Nathan Wong, a B.C.-based pharmacist who left the profession in 2024, fears witnessed dosing will overwhelm already overburdened pharmacists, creating new barriers to care.
“One of the biggest challenges of the retail pharmacy model is that there is a tension between making commercial profit, and being able to spend the necessary time with the patient to do a good and thorough job,” he said.
“Pharmacists often feel rushed to check prescriptions, and may not have the time to perform detailed patient counselling.”
Others say the return to witnessed dosing could create serious challenges for individuals who do not live close to health-care providers.
Shelley Singer, a resident of Cowichan Bay, B.C., on Vancouver Island, says it was difficult to make multiple, daily visits to a pharmacy each day when her daughter was placed on witnessed dosing years ago.
“It was ridiculous,” said Singer, whose local pharmacy is a 15-minute drive from her home. As a retiree, she was able to drive her daughter to the pharmacy twice a day for her doses. But she worries about patients who do not have that kind of support.
“I don’t believe witnessed supply is the way to go,” said Singer, who credits safer supply with saving her daughter’s life.
Melamed notes that not all safer supply medications require witnessed dosing.
“Methadone is under witness dosing because you start low and go slow, and then it’s based on a contingency management program,” she said. “When the urine shows evidence of no other drug, when the person is stable, [they can] take it at home.”
She also noted that Suboxone, a daily medication that prevents opioid highs, reduces cravings and alleviates withdrawal, does not require strict supervision.
Kendra Wong, of the B.C. health ministry, told Canadian Affairs that long-acting medications such as methadone and buprenorphine could be reintroduced to help reduce the strain on health-care professionals and patients.
“There are medications available through the [safer supply] program that have to be taken less often than others — some as far apart as every two to three days,” said Wong.
“Clinicians may choose to transition patients to those medications so that they have to come in less regularly.”
Such an approach would align with Addiction Medicine Canada’s recommendations to the ministry.
The group says it supports supervised dosing of hydromorphone as a short-term solution to prevent diversion. But Melamed said the long-term goal of any addiction treatment program should be to reduce users’ reliance on opioids.
The group recommends combining safer supply hydromorphone with opioid agonist therapies. These therapies use controlled medications to reduce withdrawal symptoms, cravings and some of the risks associated with addiction.
They also recommend limiting unsupervised hydromorphone to a maximum of five 8 mg tablets a day — down from the 30 tablets currently permitted with take-home supplies. And they recommend that doses be tapered over time.
“This protocol is being used with success by clinicians in B.C. and elsewhere,” the letter says.
“Please ensure that the administrative delay of the implementation of your new policy is not used to continue to harm the public.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle
2025 Federal Election
Poilievre to invest in recovery, cut off federal funding for opioids and defund drug dens

From Conservative Party Communications
Poilievre will Make Recovery a Reality for 50,000 Canadians
Conservative Leader Pierre Poilievre pledged he will bring the hope that our vulnerable Canadians need by expanding drug recovery programs, creating 50,000 new opportunities for Canadians seeking freedom from addiction. At the same time, he will stop federal funding for opioids, defund federal drug dens, and ensure that any remaining sites do not operate within 500 meters of schools, daycares, playgrounds, parks and seniors’ homes, and comply with strict new oversight rules that focus on pathways to treatment.
More than 50,000 people have lost their lives to fentanyl since 2015—more Canadians than died in the Second World War. Poilievre pledged to open a path to recovery while cracking down on the radical Liberal experiment with free access to illegal drugs that has made the crisis worse and brought disorder to local communities.
Specifically, Poilievre will:
- Fund treatment for 50,000 Canadians. A new Conservative government will fund treatment for 50,000 Canadians in treatment centres with a proven record of success at getting people off drugs. This includes successful models like the Bruce Oake Recovery Centre, which helps people recover and reunite with their families, communities, and culture. To ensure the best outcomes, funding will follow results. Where spaces in good treatment programs exist, we will use them, and where they need to expand, these funds will allow that.
- Ban drug dens from being located within 500 metres of schools, daycares, playgrounds, parks, and seniors’ homes and impose strict new oversight rules. Poilievre also pledged to crack down on the Liberals’ reckless experiments with free access to illegal drugs that allow provinces to operate drug sites with no oversight, while pausing any new federal exemptions until evidence justifies they support recovery. Existing federal sites will be required to operate away from residential communities and places where families and children frequent and will now also have to focus on connecting users with treatment, meet stricter regulatory standards or be shut down. He will also end the exemption for fly-by-night provincially-regulated sites.
“After the Lost Liberal Decade, Canada’s addiction crisis has spiralled out of control,” said Poilievre. “Families have been torn apart while children have to witness open drug use and walk through dangerous encampments to get to school. Canadians deserve better than the endless Liberal cycle of crime, despair, and death.”
Since the Liberals were first elected in 2015, our once-safe communities have become sordid and disordered, while more and more Canadians have been lost to the dangerous drugs the Liberals have flooded into our streets. In British Columbia, where the Liberals decriminalized dangerous drugs like fentanyl and meth, drug overdose deaths increased by 200 percent.
The Liberals also pursued a radical experiment of taxpayer-funded hard drugs, which are often diverted and resold to children and other vulnerable Canadians. The Vancouver Police Department has said that roughly half of all hydromorphone seizures were diverted from this hard drugs program, while the Waterloo Regional Police Service and Niagara Regional Police Service said that hydromorphone seizures had exploded by 1,090% and 1,577%, respectively.
Despite the death and despair that is now common on our streets, bizarrely Mark Carney told a room of Liberal supporters that 50,000 fentanyl deaths in Canada is not “a crisis.” He also hand-picked a Liberal candidate who said the Liberals “would be smart to lean into drug decriminalization” and another who said “legalizing all drugs would be good for Canada.”
Carney’s star candidate Gregor Robertson, an early advocate of decriminalization and so-called safe supply, wanted drug dens imposed on communities without any consultation or public safety considerations. During his disastrous tenure as Vancouver Mayor, overdoses increased by 600%.
Alberta has pioneered an approach that offers real hope by adopting a recovery-focused model of care, leading to a nearly 40 percent reduction in drug-poisoning deaths since 2023—three times the decrease seen in British Columbia. However, we must also end the Liberal drug policies that have worsened the crisis and harmed countless lives and families.
To fund this policy, a Conservative government will stop federal funding for opioids, defund federal drug dens, and sue the opioid manufacturers and consulting companies who created this crisis in the first place.
“Canadians deserve better than the Liberal cycle of crime, despair, and death,” said Poilievre. “We will treat addiction with compassion and accountability—not with more taxpayer-funded poison. We will turn hurt into hope by shutting down drug dens, restoring order in our communities, funding real recovery, and bringing our loved ones home drug-free.”

‘War On Coal Is Finally Over’: Energy Experts Say Trump Admin’s Deregulation Agenda Could Fuel Coal’s ‘Revival’

BREAKING: THE FEDERAL BRIEF THAT SHOULD SINK CARNEY

The Pandemic Justice Phase Begins as Criminal Investigations Commence
CHINESE ELECTION THREAT WARNING: Conservative Candidate Joe Tay Paused Public Campaign
-
2025 Federal Election22 hours ago
BREAKING: THE FEDERAL BRIEF THAT SHOULD SINK CARNEY
-
2025 Federal Election22 hours ago
CHINESE ELECTION THREAT WARNING: Conservative Candidate Joe Tay Paused Public Campaign
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoOttawa Confirms China interfering with 2025 federal election: Beijing Seeks to Block Joe Tay’s Election
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoReal Homes vs. Modular Shoeboxes: The Housing Battle Between Poilievre and Carney
-
 Business11 hours ago
Business11 hours agoHudson’s Bay Bid Raises Red Flags Over Foreign Influence
-
 2025 Federal Election8 hours ago
2025 Federal Election8 hours agoMark Carney Wants You to Forget He Clearly Opposes the Development and Export of Canada’s Natural Resources
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoHow Canada’s Mainstream Media Lost the Public Trust
-
 John Stossel1 day ago
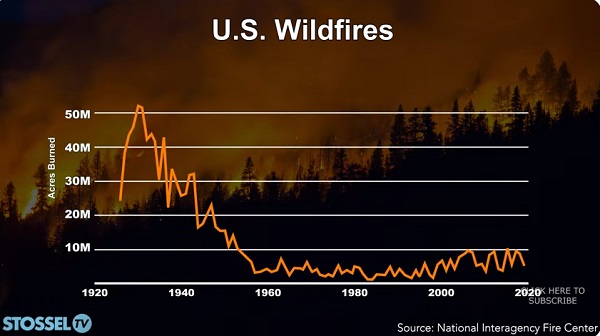
John Stossel1 day agoClimate Change Myths Part 2: Wildfires, Drought, Rising Sea Level, and Coral Reefs