Health
Prostate Cancer: Over-Testing and Over-Treatment
From the Brownstone Institute
The excessive medical response to the Covid pandemic made one thing abundantly clear: Medical consumers really ought to do their own research into the health issues that impact them. Furthermore, it is no longer enough simply to seek out a “second opinion” or even a “third opinion” from doctors. They may well all be misinformed or biased. Furthermore, this problem appears to predate the Covid phenomenon.
A striking example of that can be found in the recent history of prostate cancer testing and treatment, which, for personal reasons, has become a subject of interest to me. In many ways, it strongly resembles the Covid calamity, where misuse of the PCR test resulted in harming the supposedly Covid-infected with destructive treatments.
Two excellent books on the subject illuminate the issues involved in prostate cancer. One is Invasion of the Prostate Snatchers by Dr. Mark Scholz and Ralph Blum. Dr. Scholtz is executive director of the Prostate Cancer Research Institute in California. The other is The Great Prostate Hoax by Richard Ablin and Ronald Piana. Richard Ablin is a pathologist who invented the PSA test but has become a vociferous critic of its widespread use as a diagnostic tool for prostate cancer.
Mandatory yearly PSA testing at many institutions opened up a gold mine for urologists, who were able to perform lucrative biopsies and prostatectomies on patients who had PSA test numbers above a certain level. However, Ablin has insisted that “routine PSA screening does far more harm to men than good.” Moreover, he maintains that the medical people involved in prostate screening and treatment represent “a self-perpetuating industry that has maimed millions of American men.”
Even during approval hearings for the PSA test, the FDA was well aware of the problems and dangers. For one thing, the test has a 78% false positive rate. An elevated PSA level can be caused by various factors besides cancer, so it is not really a test for prostate cancer. Moreover, a PSA test score can spur frightened men into getting unnecessary biopsies and harmful surgical procedures.
One person who understood the potential dangers of the test well was the chairman of the FDA’s committee, Dr. Harold Markovitz, who decided whether to approve it. He declared, “I’m afraid of this test. If it is approved, it comes out with the imprimatur of the committee…as pointed out, you can’t wash your hands of guilt. . .all this does is threaten a whole lot of men with prostate biopsy…it’s dangerous.”
In the end, the committee did not give unqualified approval to the PSA test but only approved it “with conditions.” However, subsequently, the conditions were ignored.
Nevertheless, the PSA test became celebrated as the route to salvation from prostate cancer. The Postal Service even circulated a stamp promoting yearly PSA tests in 1999. Quite a few people became wealthy and well-known at the Hybritech company, thanks to the Tandem-R PSA test, their most lucrative product.
In those days, the corrupting influence of the pharmaceutical companies on the medical device and drug approval process was already apparent. In an editorial for the Journal of the American Medical Association (quoted in Albin and Piana’s book), Dr. Marcia Angell wrote, “The pharmaceutical industry has gained unprecedented control over the evaluation of its products…there’s mounting evidence that they skew the research they sponsor to make their drugs look better and safer.” She also authored the book The Truth About the Drug Companies: How They Deceive Us and What to Do About It.
A cancer diagnosis often causes great anxiety, but in actuality, prostate cancer develops very slowly compared to other cancers and does not often pose an imminent threat to life. A chart featured in Scholz and Blum’s book compares the average length of life of people whose cancer returns after surgery. In the case of colon cancer, they live on average two more years, but prostate cancer patients live another 18.5 years.
In the overwhelming majority of cases, prostate cancer patients do not die from it but rather from something else, whether they are treated for it or not. In a 2023 article about this issue titled “To Treat or Not to Treat,” the author reports the results of a 15-year study of prostate cancer patients in the New England Journal of Medicine. Only 3% of the men in the study died of prostate cancer, and getting radiation or surgery for it did not seem to offer much statistical benefit over “active surveillance.”
Dr. Scholz confirms this, writing that “studies indicate that these treatments [radiation and surgery] reduce mortality in men with Low and Intermediate-Risk disease by only 1% to 2% and by less than 10% in men with High-Risk disease.”
Nowadays prostate surgery is a dangerous treatment choice, but it is still widely recommended by doctors, especially in Japan. Sadly, it also seems to be unnecessary. One study cited in Ablin and Piana’s book concluded that “PSA mass screening resulted in a huge increase in the number of radical prostatectomies. There is little evidence for improved survival outcomes in the recent years…”
However, a number of urologists urge their patients not to wait to get prostate surgery, threatening them with imminent death if they do not. Ralph Blum, a prostate cancer patient, was told by one urologist, “Without surgery you’ll be dead in two years.” Many will recall that similar death threats were also a common feature of Covid mRNA-injection promotion.
Weighing against prostate surgery are various risks, including death and long-term impairment, since it is a very difficult procedure, even with newer robotic technology. According to Dr. Scholz, about 1 in 600 prostate surgeries result in the death of the patient. Much higher percentages suffer from incontinence (15% to 20%) and impotence after surgery. The psychological impact of these side effects is not a minor problem for many men.
In light of the significant risks and little proven benefit of treatment, Dr. Scholz censures “the urology world’s persistent overtreatment mindset.” Clearly, excessive PSA screening led to inflicting unnecessary suffering on many men. More recently, the Covid phenomenon has been an even more dramatic case of medical overkill.
Ablin and Piana’s book makes an observation that also sheds a harsh light on the Covid medical response: “Isn’t cutting edge innovation that brings new medical technology to the market a good thing for health-care consumers? The answer is yes, but only if new technologies entering the market have proven benefit over the ones they replace.”
That last point especially applies to Japan right now, where people are being urged to receive the next-generation mRNA innovation–the self-amplifying mRNA Covid vaccine. Thankfully, a number seem to be resisting this time.

From the Fraser Institute
By Nadeem Esmail and Mackenzie Moir
It’s an exciting time in Canadian health-care policy. But even the slew of new reforms in Alberta only go part of the way to using all the policy tools employed by high performing universal health-care systems.
For 2026, for the sake of Canadian patients, let’s hope Alberta stays the path on changes to how hospitals are paid and allowing some private purchases of health care, and that other provinces start to catch up.
While Alberta’s new reforms were welcome news this year, it’s clear Canada’s health-care system continued to struggle. Canadians were reminded by our annual comparison of health care systems that they pay for one of the developed world’s most expensive universal health-care systems, yet have some of the fewest physicians and hospital beds, while waiting in some of the longest queues.
And speaking of queues, wait times across Canada for non-emergency care reached the second-highest level ever measured at 28.6 weeks from general practitioner referral to actual treatment. That’s more than triple the wait of the early 1990s despite decades of government promises and spending commitments. Other work found that at least 23,746 patients died while waiting for care, and nearly 1.3 million Canadians left our overcrowded emergency rooms without being treated.
At least one province has shown a genuine willingness to do something about these problems.
The Smith government in Alberta announced early in the year that it would move towards paying hospitals per-patient treated as opposed to a fixed annual budget, a policy approach that Quebec has been working on for years. Albertans will also soon be able purchase, at least in a limited way, some diagnostic and surgical services for themselves, which is again already possible in Quebec. Alberta has also gone a step further by allowing physicians to work in both public and private settings.
While controversial in Canada, these approaches simply mirror what is being done in all of the developed world’s top-performing universal health-care systems. Australia, the Netherlands, Germany and Switzerland all pay their hospitals per patient treated, and allow patients the opportunity to purchase care privately if they wish. They all also have better and faster universally accessible health care than Canada’s provinces provide, while spending a little more (Switzerland) or less (Australia, Germany, the Netherlands) than we do.
While these reforms are clearly a step in the right direction, there’s more to be done.
Even if we include Alberta’s reforms, these countries still do some very important things differently.
Critically, all of these countries expect patients to pay a small amount for their universally accessible services. The reasoning is straightforward: we all spend our own money more carefully than we spend someone else’s, and patients will make more informed decisions about when and where it’s best to access the health-care system when they have to pay a little out of pocket.
The evidence around this policy is clear—with appropriate safeguards to protect the very ill and exemptions for lower-income and other vulnerable populations, the demand for outpatient healthcare services falls, reducing delays and freeing up resources for others.
Charging patients even small amounts for care would of course violate the Canada Health Act, but it would also emulate the approach of 100 per cent of the developed world’s top-performing health-care systems. In this case, violating outdated federal policy means better universal health care for Canadians.
These top-performing countries also see the private sector and innovative entrepreneurs as partners in delivering universal health care. A relationship that is far different from the limited individual contracts some provinces have with private clinics and surgical centres to provide care in Canada. In these other countries, even full-service hospitals are operated by private providers. Importantly, partnering with innovative private providers, even hospitals, to deliver universal health care does not violate the Canada Health Act.
So, while Alberta has made strides this past year moving towards the well-established higher performance policy approach followed elsewhere, the Smith government remains at least a couple steps short of truly adopting a more Australian or European approach for health care. And other provinces have yet to even get to where Alberta will soon be.
Let’s hope in 2026 that Alberta keeps moving towards a truly world class universal health-care experience for patients, and that the other provinces catch up.

From LifeSiteNews
Dr. Marty Makary took aim at the transgender-medical-industrial complex that has exploded in recent years during a recent press conference.
Food and Drug Administration (FDA) commissioner Dr. Marty Makary has sternly warned companies manufacturing “breast binders” to cease marketing and supplying their product to gender-confused girls seeking to make their bodies appear masculine.
“Today the FDA is taking action,” said Makary in a press conference. “We are sending warning letters to 12 manufacturers and retailers for illegal marketing of breast binders for children, for the purposes of treating gender dysphoria.”
“Breast binders are a class one medical device with legitimate medical users, such as being used by women after breast cancer surgery,” but “these binders are not benign,” he cautioned. “Long-term usage has been associated with pain, compromised lung function, and even difficulty breast feeding later in life.”
“The warning letters will formally notify the companies of their significant regulatory violations and require prompt corrective action,” said the FDA head.
.@DrMakaryFDA: “Today the FDA is taking action. We are sending warning letters to 12 manufacturers and retailers for illegal marketing of breast binders for children, for the purposes of treating gender dysphoria.” pic.twitter.com/6JNAy36223
— HHS Rapid Response (@HHSResponse) December 18, 2025
The warning letter addressed to California manufacturer, GenderBender, notes that the company’s website states that “[c]hest binding is the practice of compressing breast mass into a more masculine shape, often done in the LGBTQ community for gender euphoria.”
“Your firm should take prompt action to address any violations identified in this letter. Failure to adequately address this matter may result in regulatory action being initiated by the FDA without further notice. These actions include, but are not limited to, seizure and injunction,” advised the FDA.
During his presentation, Makary took aim at the transgender-medical-industrial complex that has exploded in recent years.
“One of the most barbaric features of a society is the genital mutilation of its children,” observed Makary.
“Pushing transgender ideology in children is predatory, it’s wrong, and it needs to stop,” he declared.
“This ideology is a belief system that some teachers, some pediatricians, and others are selling to children without their parents knowing sometimes, or with a deliberate attempt to remove parents from the decision making,” Makary explained.
To witness society “putting kids on a path of chest binders, drugs, castration, mastectomies, and other procedures is a path that now many kids regret,” he lamented, as he pointed to Chloe Cole, who has reverted to her God-given femininity after undergoing so-called “gender-affirming” surgery as a teen.
Cole is a leading voice for young people who have “detransitioned” after having medically, surgically, and socially attempted to “transition” to a member of the opposite sex.
.@DrMakaryFDA: “Pushing transgender ideology in children is predatory, it's wrong, and it needs to stop.” pic.twitter.com/TXxWNEtNZk
— HHS Rapid Response (@HHSResponse) December 18, 2025


Australian PM booed at Bondi vigil as crowd screams “shame!”

There’s No Bias at CBC News, You Say? Well, OK…

Georgia county admits illegally certifying 315k ballots in 2020 presidential election
FDA warns ‘breast binder’ manufacturers to stop marketing to gender-confused girls
-
International2 days ago
Georgia county admits illegally certifying 315k ballots in 2020 presidential election
-
 International2 days ago
International2 days agoCommunist China arrests hundreds of Christians just days before Christmas
-
 Business1 day ago
Business1 day agoSome Of The Wackiest Things Featured In Rand Paul’s New Report Alleging $1,639,135,969,608 In Gov’t Waste
-
 Energy18 hours ago
Energy18 hours agoThe Top News Stories That Shaped Canadian Energy in 2025 and Will Continue to Shape Canadian Energy in 2026
-
 Alberta2 days ago
Alberta2 days agoCalgary’s new city council votes to ban foreign flags at government buildings
-
 Business2 days ago
Business2 days agoWarning Canada: China’s Economic Miracle Was Built on Mass Displacement
-
 International18 hours ago
International18 hours ago$2.6 million raised for man who wrestled shotgun from Bondi Beach terrorist
-
 Alberta2 days ago
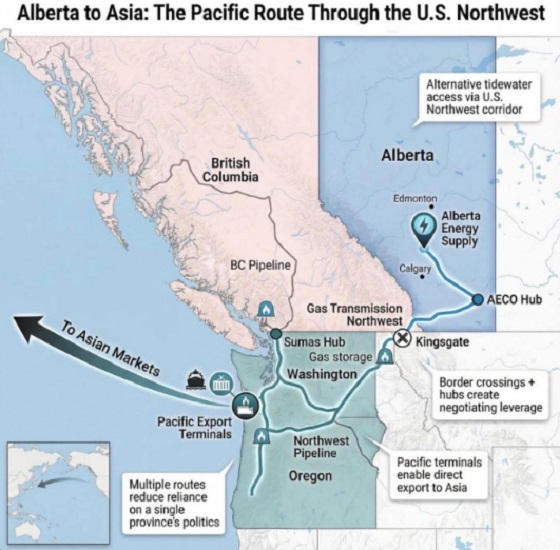
Alberta2 days agoWhat are the odds of a pipeline through the American Pacific Northwest