Health
Hundreds of Studies Show DMSO Transforms The Treatment of Cancer

The Forgotten Side of Medicine by A Midwestern Doctor
It might not be something your doctor wants to talk about, but it certainly is something we should all know more about. The video from an old 60 Minutes episode is a must see.
Dimethyl Sulfoxide (DMSO)
Exactly six months ago, I used this newsletter to bring the public’s attention to DMSO, a simple naturally occurring compound that has a number of immense therapeutic benefits and virtually no toxicity (detailed here). In turn, when it was discovered in the 1960s, it quickly became America’s most desired drug (as it cured many incurable ailments). A lot of the scientific community promptly got behind it and before long, thousands of papers had been published on every conceivable medical application for it. Consider for example this 1980 program 60 Minutes aired on DMSO:
As such, throughout this series, I’ve presented the wealth of evidence that DMSO effectively treats:
Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
A wide range of autoimmune, protein, and contractile disorders such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
A wide range of internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here).
A wide range of skin conditions such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
In turn, when I published this series (because of both how effective and easily accessible DMSO is) it caught on like wildfire, this publication went from being the ninth to top ranked newsletter in the genre, there was a nationwide DMSO shortage, and I’ve received almost two thousand testimonials from people who benefitted from DMSO (and often had remarkable results—particularly for chronic pain).

That response was quite surprising and in my eyes, a testament not only to how well DMSO works, but more importantly, how effectively DMSO’s story was erased from history (e.g., many long-time enthusiasts of natural health shared that they were blown away they’d never heard of it). This sadly illustrates how effectively the medical industry can bury anything threatening its bottom line (e.g., the FDA—for rather petty reasons—used everything at their disposal to make sure DMSO was forgotten).
In turn, within the DMSO story, I believe one of the least appreciated (or even known) facets of it are the remarkable contributions DMSO makes to the treatment of cancer—which is even more remarkable given that far more research has been done with DMSO and cancer than all the other topics I just listed. Consequently, for months I’ve wanted to publish an article on this (particularly since one incredible natural cancer therapy utilizes DMSO), but simultaneously, it just wasn’t feasible to as there was so much literature to go through.
That’s been weighing on me considerably (e.g. many readers have asked me to prioritize this article over everything else), so over the last three months (and particularly the last three weeks), I shifted my responsibilities to focus on the topic thoroughly. While it took a bit of a toll on me, the article is now done. As such, I greatly hope some of what’s in here can benefit you and I likewise thank each of you who has supported this newsletter and made it possible for me to spend so much time delving into these critical forgotten sides of medicine.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber. To see how others have benefitted from this newsletter, click here!
Story at a Glance:
- Dimethyl sulfoxide (DMSO) effectively treats a broad spectrum of conditions, including strokes, pain, tissue injuries, autoimmune inflammation, and cancer.
- DMSO inhibits cancer growth and consistently reverts cancer cells to their normal state.
- DMSO enhances cancer visibility to immune cells, enabling the body to eliminate tumors previously undetected by the immune system.
- DMSO effectively mitigates major challenges in conventional cancer care, such as radiation damage, chemotherapy toxicity, and pain from “incurable” metastatic cancer.
- DMSO markedly boosts the efficacy of many chemotherapy drugs, allowing safer, lower doses to achieve the same results.
- When paired with certain natural therapies, DMSO often produces highly effective cancer treatments, revolutionizing cancer care.
Cancer is one of the most challenging conditions to deal with in medicine, as two seemingly identical cancers can have very different causes. As a result, any standardized (holistic or conventional) protocol will inevitably fail some of the patients it is meant to treat.
Furthermore, since there is so much fear surrounding cancer (e.g., from what the primal fear brings up inside you, from how your social circle reacts to it and from how the medical system uses all of that to push cancer therapies) it is often very difficult to have a clear head about the ordeal or find the right source of advice.
Likewise, since so much money is involved (e.g. 65% of oncologist’s revenues comes from chemotherapy drugs and cancer drugs are by far the most profitable drug market), there is significant pushback (e.g. from medical boards or unhappy relatives) against anyone who attempts alternative cancer therapies making it very difficult to practice unconventional cancer care—particularly since no alternative treatment works all the time.
Note: in a recent article, I highlighted how urologists initially would not touch Lupron (which is now also used as a the puberty blocker) because of how unsafe and ineffective it was, but once they started being paid a lot of money to prescribe it for prostate cancer, it rapidly became their number one drug.
In contrast, while the conventional cancer therapies often have serious issues that make them far worse than any benefit they offer, some conventional cancer therapies are frequently the only available option which can save someone’s life (which has led to me at different times having fights with close friends or relatives either not to do chemotherapy or to get them to start it in cases where I felt it was absolutely necessary).
Given all of this, I presently believe that no “ideal” cancer treatment exists, but if it can be done (e.g., it’s effective for the cancer and feasible to implement), the most ideal to least ideal treatments are as follows:
•Identifying the root cause of a cancer, removing it, and having it quickly and permanently go away on its own (which is sometimes possible).
•Have enough time to rebalance the body so that its terrain no longer supports the cancer and the cancer can fade away on its own (which is often doable but a fairly involved process many have difficulty carrying out).
•Significantly enhance the function of the immune system so that it will eliminate the cancer.
•Find a treatment that is toxic to the cancer but relatively benign to the rest of the body.
•Find a treatment with an acceptable toxicity level and find ways to mitigate its effects.
•Accept a moderately toxic treatment with significant side effects.
•Focus on living with the cancer rather than curing it and then finding ways to mitigate the symptoms you experience both from it and any existing treatment protocols.
•Use a costly conventional therapy that is unlikely to work and live with all the side effects until your life ends (which in more extreme treatment regimens can be quite severe).
If we take a step back, what’s truly remarkable about DMSO, depending on how it is used, is that it can effectively provide most of the benefits listed above with the least amount of collateral damage (e.g., side-effects, toxicity, etc.).


 Robert W Malone MD, MS
Robert W Malone MD, MS
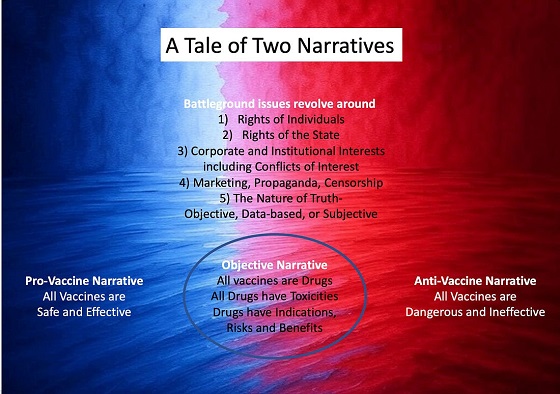
A Tale of Two Narratives
The recent West Texas outbreak of Measles has become politicized and now provides a case study of how the polarization and weaponization of politics and public health in the United States results in dysfunctional public policy. Currently, there are two major competing narratives concerning US public health policy concerning vaccines.
The Dominant Narrative
The dominant narrative, repeatedly reinforced via a wide range of channels, marketing, propaganda, and censorship – particularly during the SARS-CoV-2 outbreak- is that all vaccines, including the mRNA and adenovirus genetic therapy-based vaccines, are “safe and effective.” This typically unqualified but oft-repeated phrase has characteristics of a catechism of faith repeated by “true believers” of a vaccine-promoting cult of public health officers, academics dependent on the vaccine industry, industrial vaccinologists, the vast majority of specialist physician guilds (that universally accept funding from vaccine-manufacturing corporations), and their surrogates. Surrogates include corporate media, politicians, and academic journals that almost universally also accept significant direct or indirect funding from vaccine manufacturers. Any who question any aspect of this catechism are typically attacked, censored, and ostracized by cult members.
To illustrate with a recent example, these two terms (“safe and effective”) were repeatedly deployed and reinforced in corporate media and government messaging during the outbreak without defining or clarifying what criteria were being applied to define “safe” or “effective.” The repeated deployment and repetition of terms such as these without qualification or clarification as a key component of a public messaging campaign is a psychological manipulation tool known by the terms “neurolinguistic programming,” “natural language processing or technology,” or simply “subliminal marketing”, and relies on the use of messages designed to influence subconscious thoughts and behaviors without the audience’s conscious awareness. The use of censorship, nudge technology and other psychological manipulation methods to suppress discussion of potential harms and examination of risk/benefit/harm assessment and stratification by age and risk factors was justified as necessary to prevent “vaccine hesitancy” by the general public. Quite literally thousands of federally funded, peer-reviewed academic studies and publications examined and documented means by which ‘vaccine hesitancy” in the general public could be overcome using a wide range of propaganda, censorship, and psychological manipulation methods.
A false narrative of “vaccine hesitancy” creating risks of widespread unnecessary deaths due to infection by SARS-CoV-2 was justified, supported and promoted based on two subsidiary false narratives – 1) that SARS-CoV-2 infection was associated with a 3-4% “case fatality rate” (between 3 and 4 out of every one hundred people infected by SARS-CoV-2 would die), and 2) that the Emergency Use Authorized COVID “vaccines” were sufficiently protective to enable development of “herd immunity” if a sufficient fraction of the population would accept dosing with these products.
Like the dominant “safe and effective” narrative, these subsidiary false narratives upon which the primary dominant narrative rested were also repeated until the burden of “counterfactual” evidence became overwhelming. At that point, corporate media and government messaging was shifted to assert that these products would partially protect against severe disease and death. Strategically overlooked was that reduction in risk of severe disease and death were not listed as criteria in the Emergency Use Authorization or subsequent product marketing authorization by the US FDA. Over time, additional clinical research – notably from the Cleveland Clinic, a leading US provider of clinical services- indicated that any such benefits in reduction of clinical disease, disease severity, and death were short-lived and within weeks to months post product administration the risk of these outcomes increased relative to those that did not accept the products. This is referred to as “negative efficacy.”
In the current context of weaponization of the West Texas measles outbreak for various purposes, this dominant narrative has been repurposed and continues to be actively promoted by pivoting from COVID vaccine promotion of the childhood-focused 1960s legacy combination vaccine products Measles, Mumps and Rubella vaccines marketed as M-M-R II (Merck) and PRIORIX (GSK).
It has been my experience that the modern use of psychological manipulation (PsyWar), propaganda, censorship and marketing methods to reinforce this dominant vaccine narrative is so effective that most reporters and medical care providers do not even question whether this is true. It “feels” true to them, and therefore must be true.
In turn this profoundly influences both how front line journalists approach a ‘breaking news” story, and how medical care providers approach patient management. The baseline assumption being that if a patient that did not accept a “safe and effective” prophylactic vaccine develops a “vaccine preventable” infectious disease, then all clinical sequelae are the consequence of their failure to comply with the recommendation to accept the “safe and effective” vaccine product. The ultimate embodiment of this logic was that all who died with a positive PCR SARS-CoV-2 test during the COVID crisis died of COVID (despite any confounding medical conditions) rather than having died with COVID.
This recent post on “X” illustrates one consequence of the promotion and reinforcement of the dominant narrative in the context of measles and measles vaccines. Safe and effective. Apparently a case involving a physician who self-censors to avoid professional consequences despite being present with hard evidence of a case of vaccine-associated measles due to reversion of the vaccine strain to a disease-causing variant. Not perfectly safe and effective after all.
 |
Another example that contradicts the dominant “safe and effective” live attenuated measles vaccine narrative comes from a front-line primary care physician involved in managing West Texas outbreak-associated measles patients:
“Yes, I’ve treated fully vaccinated folks in their 20’s, 30’s, 40’s, and 50’s and even some children in Gaines County who went and got vaccinated at the health department’s recommendation and then got measles.”
Not perfectly safe and effective after all.
The Counter Narrative
The subdominant counter-narrative to “all vaccines are safe and effective” appears to have become “no vaccines are safe and effective.” This has also become a catechism for the alternative cult, one that has developed in reaction to the heavy-handed enforcement and widespread acceptance of the dominant narrative.
It should come as no surprise that this tenant of the “medical freedom movement” has developed in this way and no surprise that those who self-identify as being “medical freedom movement” warriors often self-identify as “the resistance” and will expel and delegitimize all those who reject this simplistic binary, either-or construct. This now extends even to their former champion HHS Secretary Robert Kennedy Jr., who has recently been labeled as a traitor to the cause (e.g., cult) for his statement as HHS Secretary that the best way to prevent the spread of measles is to vaccinate. This is a true statement – no alternative methods have proven to be more effective at slowing or stopping the spread of this highly infectious, very low-mortality disease. This is not the same as stating that measles vaccination is either fully safe or effective or that breakthrough cases or reversion to measles in vaccinated persons do not occur. RFK Jr. did not say that he recommended that people have their children vaccinated for measles. Yet that is what those who have accepted the counter-narrative heard, and many of them then launched campaigns to ostracize and delegitimize the HHS Secretary. Because, like in all cults, you are either for us or against us.
It is often assumed by those promoting the counter-narrative to this dominant catechism of all those who accept this storyline that all vaccines, including the childhood Measles, Mumps, and Rubella vaccines, are safe and effective have some sort of conflict of interest (COI) and that this COI extends down to individual reporters and medical care providers. In contrast, what I observe is that, although COI is rampant, in many cases, what one encounters is more akin to unthinking acceptance of the promoted dominant narrative as unquestioned truth. Or, to be more blunt, propaganda, censorship, psyops, and marketing work amazingly well on those who do not think for themselves.
Allow me to illustrate this with a recent example.
I was on a podcast discussing the West Texas measles outbreak when a phone call came in from West Texas. I responded with an automated text message that I was busy and would call back later. I immediately got a call from the same number, and I responded with another automated text message. The podcast concluded, and I called the number back. A young reporter for a West Texas-based newspaper wanted to question me about my original substack essay reporting that the “second measles death” was a second case of medical mismanagement of bacterial pneumonia. The reporter kept insisting that the hospital was saying otherwise and that this was a measles death. We went back and forth, her seeking some insight into who had tipped me off with the information that went into my initial report and my refusal to disclose my source. All of this concluded when I reprimanded her for taking the word of the hospital communications officer at face value and rather bluntly told her to seek out what was stated on the death certificate rather than relying on hospital PR at a time when the hospital was at risk for a medical malpractice/wrongful death lawsuit. I knew that neither the reporter nor the hospital had seen the death certificate because I knew that no death certificate had been issued at this time. However, it illustrated that, just as the managing physicians in the hospital had been biased by the dominant narrative regarding measles and measles vaccination, this young reporter had accepted that narrative without questioning the facts of the case. I very much doubt either the reporter or the managing physicians had accepted Pharma dollars to promote the dominant vaccine narrative. Still, they had become inadvertent allies in advancing and reinforcing that narrative.
The Sins of Binary Thought within the State
We are living in a time when virtually all issues in politics and public health are framed as binary. There is a right way or a wrong way to think. But life, science, and medicine are not binary, but rather more of a nuanced spectrum of information, ideas, opinion and truth. When framed as either A or B, then it becomes impossible to have a productive discussion or to negotiate nuanced public policy. And as if that is not bad enough, we are also living in a time when the State has assumed a role historically played by centralized religion. The State has assigned to itself the role of being arbiter of truth, to such a degree that information collected by the State which contradicts the approved truth will be suppressed. Suppose you find this discordant with your view of the State as a fair and balanced actor. In that case, I recommend that you look into the manipulation and deletion of adverse event data associated with the COVID genetic therapy-based products by those managing the Defense Medical Epidemiological Databased (DMED) or the CDC VAERS system.
The consequence of this simplistic, binary way of thinking, combined with the State assuming the role of being the ultimate arbiter of truth, is a sort of mass groupthink that creates barriers to effective policy decision-making in all aspects of political life. The consequences in public health are particularly stark and visible, but the same forces extend across the entire range of public policy.
Is There Another Way?
Both the pro-vaccine and the anti-vaccine cults will launch a withering social media firestorm on anyone who takes this position, but the inconvenient truth is that vaccines are helpful in some situations and not valuable for others. All vaccines, like all drugs, have side effects. In many cases, most if not all authorized vaccines have some degree of efficacy against the disease or infections they are purported to prevent. The issue should not be a binary argument between pro- vs anti-vaccine. This real issues are:
- What are the actual data supporting or refuting the usefulness of each individual vaccine? The true safety, effectiveness, and risk/benefit/harm analyses of each product stratified by age and co-morbidity. The only way to determine this is with solid, unbiased data, analyzed by people and processes that are free of bias. Fortunately or unfortunately, depending on your point of view, the COVID crisis has revealed and documented that open, transparent collection and analysis of the necessary public health and clinical trial data describing key safety and effectiveness characteristics of virtually all vaccines are not available. Furthermore, solid data on the true incidence and risks of virtually all “vaccine preventable” diseases are not available. Data gathered in compliance with modern standards, and with availability of modern medical care norms such as antibiotic treatment of secondary bacterial infections. Without such data, a valid assessment of risk/benefit stratified by age and co-morbidity is impossible. And so any statement that a given vaccine is either “safe and effective” or the contrary is invalid.
- Does the State have the right to impose a medical procedure on an individual without informed consent? Speaking personally, this is the issue that really got me fired up at the beginning of the COVID genetic therapy-based intervention campaign. I was under the illusion, reinforced by decades of training as a clinical researcher, regulatory specialist, and bioethicist that this had been decided by the post-WWII Nuremberg trials, US Belmont report, and the rich literature of modern clinical research bioethics. But this body of legal precedent, public policy, and academic study was thrown in the ash can at a moment’s notice in the face of the promoted false narrative of a severely inflated infectious disease threat. When this issue has been referred to the US Judiciary in various forms, it has predominantly acted to support the Murray Rothbard thesis that the role of the Judiciary is to support and legitimize the State. The Judiciary has not acted to ensure justice for those harmed, and it has not acted to support fundamental constitutional tenants concerning the rights of individuals. This issue must become a major focus of political discourse, but the constant framing of any related discourse as either pro- or anti-vaccine prevents this from happening.
In Conclusion
My advice? Take a step back and take a deep breath. Don’t get distracted by the chaos and promoted binary narratives. These artificially promoted cult-like positions primarily act to maintain stasis and prevent effective policy discussion and decisions. In other words, developing and driving cult-like behavior in support of extremist positions primarily serves to maintain status quo. This is likely to be intentional in a world where PsyWar techniques and technologies have become the norm.
The way out of the woods is to allow and enable objective, unbiased data to be gathered and analyzed. Then, make public health policy decisions based on those data. The current data are biased in various ways, and the interpretation of those data has not been objective or free of COI. In the meantime, neither trench warfare nor circular firing squads will permit or support effective public health policy decisions.
By the way, that happens to be the position taken by HHS Secretary Robert F. Kennedy Jr. to the best of my knowledge. We need more data, we need time to gather and analyze those data, and in the interim, we need to avoid exacerbating and inflaming the situation by yet more hasty, arbitrary, and capricious decision-making.
And we need the Judiciary to step up and defend the Constitution and individuals’ rights to bodily autonomy in a non-partisan manner.
Malone News is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
Invite your friends and earn rewards


I have long reviewed medical records of patients harmed by poor medical care. Here, I present clear evidence of what actually caused the 2 girls deaths in Texas. It wasn’t measles.
Before I start, I want all to know that the parents of both children are from the same community and know each other. They and the community are obviously in grief over these unnecessary and easily preventable deaths, which you will learn more about why below. I will state at the outset that, in my professional opinion, neither child died of measles. Not even close.
CASE #1 – Kaley Fehr, Age 6
I will only briefly discuss Kaley’s case because it was already covered extensively in an interview I did with CHD TV a little over two weeks ago. Plus, the record and findings are straightforward.
Kaley was a six-year-old previously healthy girl who contracted measles along with her four siblings (all of whom weathered the illness just fine under the care of Dr. Ben Edwards). As her rash was clearing, she began to develop signs and symptoms of “secondary bacterial pneumonia,” a not uncommon complication of almost any viral infection. To wit, one of my three daughters fell ill with the same after she contracted influenza at age 14; however, in her case, she recovered from it two days after receiving an appropriate antibiotic.
In Kaley’s case, her worsening respiratory status led her parents to bring her to Providence Covenant Children’s Hospital in Lubbock, Texas, on 2/22/25 at 12:08 PM.
The hospital correctly diagnosed her with secondary bacterial pneumonia and then treated her with two antibiotics, ceftriaxone and vancomycin. This was a blatant deviation from the standard of care in treating hospitalized patients with “community-acquired pneumonia (CAP),” the guidelines for which have long recommended a different combination, e.g., ceftriaxone and azithromycin (or a quinolone).
Only azithromycin and quinolones cover mycoplasma pneumonia, a prevalent cause of community-acquired pneumonia (this is why the guidelines recommend them). Neither ceftriaxone nor vancomycin will treat mycoplasma because they work by disrupting the cell walls of bacteria. Mycoplasma does not have a cell wall.
Vancomycin, the antibiotic they chose instead of azithromycin, is used to treat “hospital-acquired pneumonia” as it is one of the only antibiotics that covers MRSA (methicillin-resistant staph aureus). This common organism inhabits hospitals and medical facilities. Kaley was from a rural Mennonite community and had not been in any hospital.
Despite her persistent and increasing deterioration in respiratory status, which eventually led to requiring intubation and mechanical ventilation, this deviation from the standard of care went unnoticed and uncorrected until just over a day before she died, when the test for mycoplasma returned as “positive.”
Azithromycin was then immediately ordered. However, from the chart, it appears it took ten hours before she received her first dose (documentation of the exact time may be missing). She was dead less than 24 hours later, 4 days after being admitted. The time of death was 06:43 on 2/26/25. My opinion as to the cause of death is that it was from an overwhelming lung injury called Acute Respiratory Distress Syndrome (ARDS) caused by mycoplasma pneumonia. The sole reason why she died from mycoplasma was because the initial antibiotic regimen violated the standard of care in the treatment of hospitalized community-acquired pneumonia because they neglected to treat her upon admission with azithromycin (i.e., a “Z-Pak deficiency”).
Note that azithromycin has excellent penetration into lung tissues and is highly effective at treating mycoplasma. Again, had they started azithromycin on Day 1, as has been recommended for decades, she would still be alive today.
The above findings were articulated in my interview with CHD TV on 3/19/25 but were subsequently ignored and/or distorted by the mainstream media. A reporter from USA Today reached out to Rebuild Medicine (my new non-profit) with questions. This is the exchange between my Executive Director and the reporter:
 |
 |
The above text also included links to several CAP guidelines, yet, in the USA Today article that was subsequently written about the case, the reporter 1) took a swipe at my credibility by describing me as a misinformationist, 2) did not even mention the treatment guidelines for community-acquired pneumonia that we had sent him, and 3) included parts of this below statement that the hospital released in response to my video interview. The mendacity of the below statement is astonishing:
“A recent video circulating online contains misleading and inaccurate claims regarding care provided at Covenant Children’s. Patient confidentiality laws preclude us from providing information directly related to this case. What we can say is that our physicians and care teams follow evidence-based protocols and make clinical decisions based on a patient’s evolving condition, diagnostic findings, and the best available medical knowledge. Measles is a highly contagious, potentially life-threatening disease that often creates serious, well-known complications like pneumonia, encephalitis and more.”
CASE #2 – Daisy Hillebrand, Age 8
I received Daisy’s medical records this past Monday via email at 5:55 p.m. Intrigued, I immediately dove in. I began reviewing and taking notes in an Excel spreadsheet because the records were not chronological. The printouts of the electronic medical record totaled 291 pages and came in 6 separate PDF files. It represented the total record for two separate admissions to the ICU of University Medical Center and one to Providence Covenant Children’s Hospital, all again located in Lubbock, Texas.
I worked continuously from 6 p.m. until 1:45 a.m., then put in another 2.5 hours more in the morning. Up until approximately midnight, my working impression of the cause of Daisy’s death was that it indeed was from measles pneumonia. Only after I opened and began reviewing the last file did I find data directly contradicting that impression. I had that initial impression because that was the “working diagnosis” of the ICU team, as documented in their daily notes.
In this case, I will start with my determination of the cause of death in the last admission. Then, I will provide details of the multiple poorly managed hospitalizations (understatement) that she suffered over the 4 weeks leading up to her death.
Cause of death: ARDS secondary to hospital-acquired pneumonia caused by a highly antibiotic-resistant E.Coli “superbug.” Based on the progression and trajectories of her illness, I believe that she contracted the infection from her first ICU admission, which is what caused her to return to the ICU 2 days after that discharge.
One of the tragedies (there were multiple) of this case is that the ICU team in charge of her care when she was re-admitted never considered the possibility of hospital-acquired pneumonia (HAP) until day 6 of 8. For an adult ICU specialist admitting a patient with an infection who was just discharged from an ICU, empiric treatment for hospital-acquired organisms is so basic and routine; I was shocked they did not do this.
In a minor defense of the pediatric team caring for Daisy, there are no published national treatment guidelines with specific antibiotic recommendations for the empiric treatment of hospital-acquired pneumonia (I did find one from the University of North Carolina (UNC), however). The first adult guidelines for HAP were published by the American Thoracic Society in 2005. Here we are 20 years later, and, aside from UNC, the field of pediatrics has not gotten around to doing the same. I found a paper by the Cochrane Library that proposed the methodology for creating one, but although published in 2019, it has not been completed yet. The American Academy of Pediatrics should be ashamed.
The problem for the hospital is that the absence of a treatment guideline is not why she died because had they sent a sputum culture on admission, by Day 3, they would have not only identified the organism but would have learned the antibiotic it was sensitive to and could have started it immediately. Her death on Day 8 would have likely and easily been prevented. Although they did send a urine culture, a blood culture, a viral PCR respiratory panel, and a PCR for MRSA and Staphylococcus (all of which were negative), they did not send a sputum culture. For a pneumonia.
For the sake of brevity, each time I detail a deviation from the standard of care in the below review of all three hospital stays, rather than explaining why it violates the standard in depth (and because I trust it will be evident to even laypeople), I will use baseball terminology by writing “strike” to indicate that “they missed the ball.” The failure to send a sputum culture in a patient with pneumonia who recently spent days in an ICU is Strike 1.
The failure to send a sputum culture had another tragic consequence – it allowed the care team, based on the viral respiratory panel being negative (which does not include measles PCR, by the way), to instead 1) assume that measles was the underlying cause on Day 2 and then, 2) immediately stop antibiotics in a seriously ill and infected child. Strike 2.
In the 8 days of her second hospital admission, she only received 5 days of antibiotics, and that is because, despite a rising white cell count in her blood, they did not restart antibiotics until Day 4, when she spiked yet another fever (Strike 3).
Further, during the three days Daisy received no antibiotics, she was given high-dose steroids. Please know that steroids, when paired with appropriate antibacterials, improve outcomes in pneumonia, but giving them without worsens outcomes. They presumably did this because their working diagnosis was “measles pneumonitis,” not bacterial pneumonia. The doctor in charge kept writing things like: “severe pulmonary sequela of measles infection around 3 weeks ago” and “we are concerned that the true extent of her lung injury due to measles is unknowable and it may be an end-stage process given the span of illness and the fact she truly is an outlier.” I don’t know what that last part means except that the clinical reasoning is unclear, and a broader “differential diagnosis” was not generated. At all.
Know that I have long taught my ICU residents and fellows the two guideposts that governed my care plans for critically ill patients. The first is, “If what you are doing is working, keep doing what you are doing.” This means that if their clinical trajectory was one of slow or steady improvement, sending endless diagnostic tests or adding therapies just because they were still ill is most often unnecessary.
The other was, “If what you are doing is not working, change what you are doing.” In this situation, I would re-review all the clinical data and further explore any causes I might be missing, or I would add on treatments that, although not standard, might offer benefit. I would try anything that might turn someone around, as long as the risk/benefit profile was favorable (when someone is persistently deteriorating, risk/benefit ratios change rapidly such that almost any treatment that holds the possibility for benefit is worthwhile to prevent death). In my opinion, at least.
With that in mind, I will say that I was encouraged by the one instance I found of the team “thinking outside the box” and trying a somewhat experimental treatment. They decided to give her intravenous immunoglobulin (IVIG)! One trial from China in 2015 found that IVIG improved outcomes in children with severe pneumonia (not measles-specific), and another study found that IVIG batches tested in 2021 contained measles-neutralizing antibodies. Good for them for trying something “off protocol.” Problem: they did not give her the IVIG until Day 7, one day before death.
Also, it was not until one day after re-starting antibiotics (Day 6) that they sent a sputum culture (Strike 4 – standard practice is to send a culture at the same time you start antibiotics). This was also the first time the thought that she might have HAP appeared in the record. This thought led them to then change her antibiotic to one that is routinely used for possible HAP (ceftazidime). Problem: The adult guidelines would have dictated that they start Imipenem or Meropenem, but since they don’t have a pediatric guideline published yet, I will not give them a strike for this.
Two days later, on Day 8, she died of refractory hypoxemia – they could no longer get oxygen into her blood via her lungs despite numerous heroic mechanical ventilation maneuvers. This, to me, is a condition that is akin to drowning in pus.
A few hours after her death, the sputum culture they sent on Day 6 was reported in the record (this is what caused me to change my working diagnosis as to the cause of her pneumonia). My jaw dropped as I read it: It showed 4+ growth of “E.Coli,” a nasty bug generally found in our GI tract only. If you don’t know what 4+ means, see this chart below, which explains the “semi-quantitative growth scale” for bacterial cultures:
 |
If you think this can’t get any worse, you would be wrong: next came the panel of susceptibilities to a slew of antibiotics. Read it and weep:
Ampicillin – Resistant, Ampicillin/Sulbactam – Resistant, Aztreonam – Resistant, Cefazolin – Resistant, Cefepime – Resistant, Cefoxitin – Resistant, Ceftriaxone – Resistant, Cefuroxime- Resistant, Ciprofloxacin – Resistant, Levofloxacin – Resistant, Piperacillin – Resistant, Tetracycline – Resistant, Tobramycin – Resistant, and finally and tragically, Ceftazidime- Resistant.
It was sensitive to only a handful of antibiotics, one of which was meropenem, which is what would have been recommended by the Adult HAP Guidelines. Daisy had numerous risk factors for HAP (previous antibiotics, previous ICU, immunosuppressed, really sick, mechanically ventilated). In conclusion, an appropriate differential diagnosis for her pneumonia did not occur until Day 5, and a sputum culture was sent too late for them to discover that the antibiotic they selected was resistant to the organism she died from.
I am going to temporarily interrupt this post to warn you that, in the below reviews of the two hospital admissions she underwent in the week before the above “final” one, the above pattern of error-prone care and missed opportunities to save her life will continue.
HOSPITAL ADMISSION AT UMC 2 DAYS BEFORE THE FINAL ICU STAY
In this hospitalization, which began on 3/21/25, 6 days before the above admission, Daisy presented with typical symptoms of pneumonia along with a chest x-ray showing a left lower lobe process, classic for bacterial pneumonia. Her admitting diagnosis was “viral illness with probable secondary bacterial pneumonia.” Just like in Kaley Fehr’s case at Covenant Hospital, at UMC, they also decided to treat Daisy with the same inexplicable and standard-violating combination of ceftriaxone and vancomycin. Strike 1. However, Daisy did not suffer the same fate as Kaley because whatever bug was making her ill at this point, it appeared that it was sensitive to this combination, plus her mycoplasma test was negative. Near miss though. Not all medical errors lead to harm, and malpractice cannot be established without harm.
Although the mother was not aware that Daisy had a subtle rash on her back on admission, the ER physician suspected it was measles and sent off a PCR test, which returned positive on the day of discharge. OK, so she had measles too.
She was pretty sick lung-wise at first because she required admission to the ICU for oxygen support. However, her oxygen requirements decreased pretty quickly, her appetite improved, her rash began to “heal and fade,” and she was discharged home on oral antibiotics on Day 4. They prescribed her oral cefdinir, which was a fine choice, in my opinion, because she had responded to ceftriaxone in the hospital (a similar antibiotic).
Problem: in the discharge note, the doctor documented that “the parents appeared concerned” with the discharge and then reported that he/she had “reassured them.” Privately, Daisy’s father told me that was the same day her measles test came back positive, and he thinks that is why they sent her out so quickly. He felt she “didn’t look too good” and was concerned. I would have to agree with him based on the fact that she quickly began to get worse upon arriving home such that 2 days later, on 3/26/25, she had to return to the ER to be readmitted with what turned out to be the fatal E.Coli pneumonia episode I detailed above. My thought: she was beginning to fall ill with E.Coli pneumonia as she was being discharged (resistant to the cefdinir she left with).
I hope you have noticed that I have not overused the phrase, “If you think that was bad, it only gets worse.” If you allow me, I will invoke that phrase again here. Read on:
ADMISSION TO COVENANT HOSPITAL TWO DAYS PRIOR TO THE ABOVE UMC ADMISSIONS
If the sequence of events is confusing because I am “going back in time,” let’s change it up and start from the beginning so I can provide you with the timeline from the beginning of her illnesses.
Daisy had a history of chronic tonsillitis and was being scheduled for a tonsillectomy. A month before her death, as per Dr. Richard Bartlett, Daisy was diagnosed with mononucleosis and developed persistent fevers, which continued throughout the month, including all her hospital admissions. Daisy’s father told me that at one point in the first few weeks, she was also diagnosed and treated for strep at another facility, which Dr. Bartlett thinks was Seminole Hospital District (I don’t have the records for that visit). Then, late in the third week of her illnesses, she was admitted to Covenant Children’s Hospital in Lubbock, stayed one night, and was discharged. 2 days later, she was admitted to UMC for the first of her two hospital admissions there. We good with the timeline?
Now, we have to talk about what happened during her one-night stay at Covenant because had she been appropriately treated there, she would never have ended up at UMC, and all of the above would have been avoided.
Briefly, on 3/18/25, she was at a community health clinic where they found her to require oxygen, so she was sent to the ER. She complained of difficulty breathing, abdominal pain, nausea, and inability to eat and was found with thrush on exam. She had a recent Tmax of 103.7. A CT scan of the abdomen and chest was done, which found splenomegaly and a left lower lobe pneumonia surrounded by a small amount of fluid (e.g., a pleural effusion).
She was given IV ceftriaxone (no azithromycin – Strike), corticosteroids, a breathing treatment (albuterol), and a painkiller (Toradol). This was in the ER, and I do not have the records from the ER, just the hospital stay. She was then admitted to Covenant Children’s Hospital with the diagnosis of pneumonia with a “plan to transition to oral antibiotics in the a.m.” Strike 1 for the absence of azithromycin in her regimen. Again. 3rd hospital this has happened at in my reviews of these cases (someone please call the Department of Health in Texas). No sputum culture was ordered, although a blood culture was. Strike 2.
She was given oral amoxicillin and IV ceftriaxone (unnecessarily redundant coverage but not a strike), Motrin, and Tylenol (ugh, but not a strike). By the next day, her oxygen levels had improved, and she was eating OK, so they discharged her. Problem: the only medication she was discharged with, per the record, was the anti-fungal drug nystatin for the thrush. No antibiotics for her pneumonia. Strike 3, and I really mean Strike 3.
What? The only possible defense is that someone forgot what the CT showed (it appears the ED is separate from the hospital) and instead went by the chest X-ray (CXR) they did in the hospital. Why you would do a CXR on the same day she had a CT is beyond me (CTs are much more sophisticated and detailed).
I suspect the CXR caused the problem because it only revealed bronchial wall thickening. It missed the lower lobe process seen on CT, which is not uncommon as CXRs are much less sensitive to diagnosing pneumonia than CTs. The radiologist stated in his report that “bronchial wall thickening can be seen in asthma or viral illnesses.”
Below is the email with my preliminary findings that I sent to Brian Hooker, Chief Scientific Officer at Children’s Health Defense
I did a quick review, not detailed, but this is what I came up with, and I am again absolutely gobsmacked:
1) I can find no lab work in the chart; it appears from her discharge they did not do any
2) The admission note mentions a CT of the abdomen and chest. The CT abdomen revealed splenomegaly, and the CT Chest revealed a lower lobe opacity and a small pleural effusion. The reports are not included; I think they were done in another facility. The CT is diagnostic of bacterial pneumonia ( focal process with an effusion—i.e., not viral).
3) She was given antibiotics while in hospital but not upon discharge
OVERALL IMPRESSION: Left lower lobe bacterial pneumonia and thrush indicating an immunosuppressed status. They gave her one day of antibiotics for this bacterial pneumonia and then discharged her without an oral antibiotic regimen. She was discharged on 3/19. Two days later (3/21) was her first hospitalization to UMC… for a left lower lobe pneumonia, which landed her in the ICU. To me, this is a clear case of a “missed diagnosis.” Had she been given appropriate oral antibiotics upon discharge, the slow-moving train wreck at UMC would likely have been avoided. There are no words for this. I advise any parent or guardian of a young child to move from that area of Texas immediately in the event they ever need competent medical care. This is almost certainly a separate instance of medical malpractice for which this hospital and its pediatricians could be held liable.
Can you guys find out where the CAT scans were done and get records from that visit? It sounds like it was an outside ER or free-standing ER.
My short, narrative summary of what happened to poor Daisy:
Daisy became ill with mononucleosis a month before death, soon followed by a strep infection and then thrush. Fevers persisted throughout, and then three weeks after the mono diagnosis, she was admitted to Covenant Childrens, diagnosed with left lower lobe pneumonia, and treated successfully. However, she was sent home without oral antibiotics. Unsurprisingly, 2 days later, she was admitted to UMC’s ICU with measles and a worsening left lower lobe pneumonia, which was again, despite errors in antibiotic selection, successfully treated, and she was discharged despite concerns by her parents. The measles rash was clearing at this point. Then, 2 days after that, she was re-admitted to UMC’s ICU with a worsening CXR (now involving her right lung) and severely worsened oxygenation. Instead of suspecting a severe hospital-acquired bacterial infection and sending a sputum culture, the presumptive diagnosis was that her lungs were failing from measles pneumonia, and her antibiotics were stopped. She was instead given corticosteroids for “measles pneumonitis.” She continued to deteriorate despite their re-starting antibiotics on Day 4 and giving IVIG on Day 7. She died on Day 8 of what a few hours later was discovered to be a large amount of E.Coli in her sputum that was highly resistant to the antibiotics she was on.
I largely (and atypically for me as a writer) left out the many emotions I felt while writing this review. I will write a separate post to explore my thoughts about these two cases and why I think hospital care is deteriorating throughout the country, and not just in pediatrics. Recent papers have documented significant decreases in Americans’ trust in their hospitals and doctors (and media) compared to before Covid.
Further, these cases are being widely and repeatedly portrayed as “measles deaths” by a pharma-controlled press in an attempt to regenerate enthusiasm for vaccines (IMO by instilling exaggerated fears of measles (over 90% of measles cases are benign, and most complications can be easily treated with competent medical care). If the media continues to do this fear-mongering by using cases of non-measles deaths, public trust will plummet even further (or maybe I should say public distrust will skyrocket further).
I want to thank Dr. Ben Edwards and Dr. Richard Bartlett, who are in Lubbock doing everything they can to keep kids out of the hospital by delivering appropriate and effective outpatient care.
If you appreciate the pro-bono time and effort I put into performing these extensive case reviews and
researching and writing my posts, please consider a paid subscription.

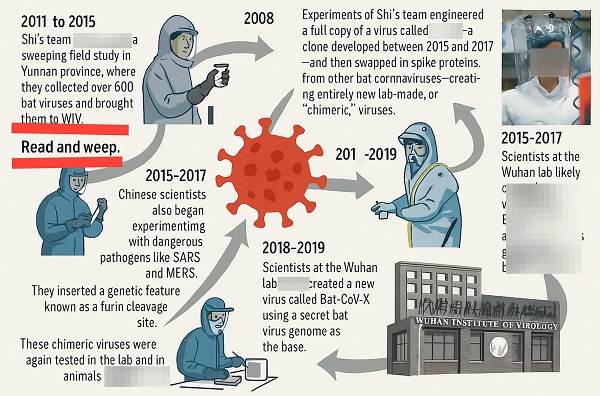
BLOCKBUSTER REPORT: Canada’s ties to Wuhan Institute of Virology and creation of COVID uncovered by Sam Cooper of The Bureau

Researchers Link China’s Intelligence and Elite Influence Arms to B.C. Government, Liberal Party, and Trudeau-Appointed Senator

Hong Kong Detains Parents of Activist Frances Hui Amid $1M Bounty, Echoing Election Interference Fears in Canada

RCMP memo warns of Chinese interference on Canadian university campuses to affect election
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoMark Carney Vows Internet Speech Crackdown if Elected
-
 2025 Federal Election24 hours ago
2025 Federal Election24 hours agoPPE Videos, CCP Letters Reveal Pandemic Coordination with Liberal Riding Boss and Former JCCC Leader—While Carney Denies Significant Meeting In Campaign
-
 2025 Federal Election14 hours ago
2025 Federal Election14 hours agoASK YOURSELF! – Can Canada Endure, or Afford the Economic Stagnation of Carney’s Costly Climate Vision?
-
 Freedom Convoy2 days ago
Freedom Convoy2 days agoA Miscarriage of Justice
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoTrudeau and Carney Have Blown $43B on EVs
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoPoilievre will make it harder for politicians to boost their portfolios, close Carney loopholes
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoMark Carney To Ban Free Speech if Elected
-
2025 Federal Election12 hours ago
CSIS Warned Beijing Would Brand Conservatives as Trumpian. Now Carney’s Campaign Is Doing It.