Health
Hundreds of doctors resign from British Medical Association over its support for puberty blockers

From LifeSiteNews
Hundreds of U.K. doctors are resigning from the British Medical Association over its opposition to a ban on puberty blockers for kids, accusing the union of ignoring evidence-based medicine and failing to represent its members’ views.
According to reports in The Times and The Telegraph, hundreds of doctors are not only going public to express their anger with the British Medical Associations’ decision to reject the Cass Review’s findings on the dangers of puberty blockers – and many are resigning.
According to The Telegraph: “Doctors with decades of experience have resigned from the British Medical Association because of the union’s opposition to the Cass review.”
As I reported earlier in this space, on August 1 the British Medical Association – the U.K. doctor’s union – called on the government to lift the ban on puberty blockers for minors and called for a pause on the implementation of the National Health Service’s Cass Review.
Initially, 1,000 senior physicians from across the U.K. responded by publishing an open letter to chairman of the BMA, Professor Philip Banfield; that number is now up to 1,400, with 900 of those being BMA members. Among their accusations is that the 69-member council passed their policy at a “secretive and opaque” meeting.
READ: Texas forbids changing sex on driver’s licenses, state IDs for ‘gender identity’
“We write as doctors to say, ‘not in my name,’” the letter read. “We are extremely disappointed that the BMA council had passed a motion to conduct a ‘critique’ of the Cass Review and to lobby to oppose its recommendations … It does not reflect the views of the wider membership, whose opinion you did not seek. We understand that no information will be released on the voting figures and how council members voted. That is a failure of accountability to members and is simply not acceptable.”
The letter further stated that the Cass Review “is the most comprehensive review into healthcare for children with gender related distress ever conducted” and urged the BMA to “abandon its pointless exercise” of attacking and opposing the recommendations.
“By lobbying against the best evidence we have, the BMA is going against the principles of evidence-based medicine and against ethical practice,” the doctors wrote, in an almost unprecedented broadside against their own union in protest of the BMA’s brazen transgender activism.
As first reported by The Times, comments made beneath that open letter “reveal many doctors have torn up their membership cards in response to the union’s stance on the review.” One commenter stated: “On the basis of the BMA’s outrageous stance on the superbly researched and written Cass Report, which has my full support and endorsement, I have decided to leave the BMA having been a member for 50 years since I qualified as a doctor. Increasingly, they not only fail to represent my views, they display no respect for the very premise and ethos inherent in being a medical professional.”
Another doctor wrote: “As a union, primarily, it is the role of the BMA to represent its members, and not to drive clinical opinion, especially in specialist areas. I am considering resigning after membership of 42 years.” A third stated: “I left the BMA partly because of this sort of behaviour on the part of the leadership, having been a member for some thirty years.” Jacky Davis, a consultant radiologist and council member, told The Times:
This minority has voted to block the implementation of Cass, an evidence-based review which took four years to put together. They have no evidence for their opposition. The Cass review is not a matter for a trade union. It is not our business as a union to be doing a critique of the Cass review. It is a waste of time and resources.
READ: Federal court backs Christian teacher who refused to call kids by transgender ‘identity’
GB News also reported on the exodus, reporting that: “Critics slammed the decision as not representing the views of all members, critiquing the BMA’s ‘abysmal’ leadership which was becoming ‘increasingly bonkers and ideologically captured.’” And according to the Daily Mail: “One signatory called for a ‘vote of no confidence in BMA leadership’ and another commenting that ‘activists appear to have been allowed to take over.’”
What is so extraordinary about this is that LGBT activists have achieved phenomenal success by infiltrating and taking over organizations, and then imposing their agenda from the top-down. Once LGBT activists are in a position to pass policies, control votes, and even censor publications, their agenda is assured. This has been incredibly effective for decades.
In this instance, however, the ideologically captured British Medical Association is facing a full-scale revolt from its own members, and its credibility is taking a severe hit. Even the press coverage of their move, which would have been laudatory only a few years ago, is almost universally negative.
The BMA is still committed to its agenda – but its grip on the narrative has been broken, and it seems unlikely that the union will be able to reestablish it.

Alberta
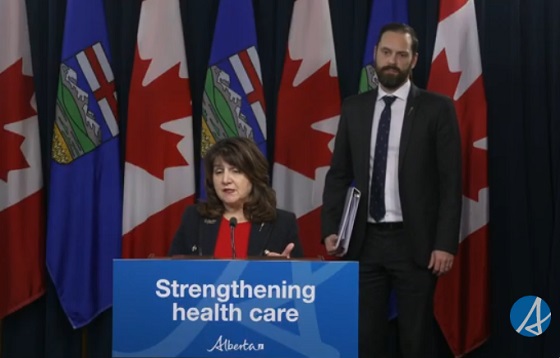
Alberta introducing dual practice health care model to increase options and shorten wait times while promising protection for publicly funded services
Enhancing access through dual practice
If passed, Bill 11, the Health Statutes Amendment Act, 2025 (No. 2), would modernize physician participation rules to give doctors flexibility to work in both the public system and private settings. Dual practice would allow physicians to continue providing insured services through the provincial health insurance plan while also delivering private services.
Alberta’s government has looked to proven models in other jurisdictions to guide the development of a model that strengthens access while safeguarding the public system. Dual practice exists in New Brunswick and Quebec and is widely used in countries with top-performing health systems, including Denmark, the Netherlands, United Kingdom, France, Germany, Spain and Australia.
“For years, governments across Canada have tried to fix long wait times by spending more money, yet the problem keeps getting worse. Alberta will not accept the status quo. Dual practice gives us a practical, proven tool that lets surgeons do more without asking taxpayers to pay more. It means shorter waits, better outcomes and a stronger health system for everyone.”
If passed, this dual practice model would be closely monitored to protect Alberta’s public health care system. The government, for example, would ensure that dual practice physicians maintain separate records for the services they provide, so no public funding subsidizes private services.
Bill 11 would include provisions to restrict participation, which could include:
- Mandating that surgeons in dual practice must perform a dedicated number or ratio of surgeries in the public system to be eligible to perform surgeries privately.
- Restricting specialties to public practice if shortages would compromise public care.
- Potentially restricting private practice to evenings, weekends or to underutilized rural sites, as required.
Alberta’s government remains committed to its public health guarantee: No Albertan will ever have to pay out of pocket to see their family doctor or to get the medical treatment they need. These proposed changes comply with the Canada Health Act.
Alberta’s government is also committed to getting Alberta’s dual practice model right and to taking a thoughtful approach to ensure the best path forward. At this time, family medicine providers will not be eligible to be flexible participants within this new model. The priority is to focus on making sure all Albertans have access to a primary care provider. Additionally, surgeries for life-threatening conditions such as cancer and emergency procedures will remain entirely publicly funded with no private option available.
“Albertans are waiting too long for the health care they need, so we are taking bold and decisive action to shorten wait times, increase access and give Albertans more choices over their own health care. At the same time, we will continue building a strong public health system where no one is denied access to the services they need because of an inability to pay.”
If passed, Bill 11 would create new options for doctors and patients. It would expand Alberta’s health system to provide more care by allowing doctors to treat more patients. Each time a patient chooses to pay for care in a private clinic or a clinic operating on evenings and weekends, for example, resources would be freed up so another patient could receive publicly funded care. This proposed new model would also support physician attraction and retention.
“As dual practice enhances flexibility for Albertans, physicians and medical professionals, safeguards will be established and utilized to protect and grow hospital and public health system capacity.”
“Albertans deserve choice and timely access to safe care, whether in a private or public setting. With the creation of the dual practice model, we can extend treatment options to patients while helping hospitals focus their resources on the highest-acuity patients.”
“I believe all options to improve access to health care for Albertans should be on the table. Therefore, the government’s dual practice legislation is a welcome option. Appropriate guardrails must be in place to ensure the spirit of the Canada Health Act is maintained.”
Quick facts
- Physicians would continue to bill the provincial plan for public services and may offer private services separately.
- Physicians may still choose to work entirely in public or entirely in private settings.
Proposed legislation would modernize physician rules, drug coverage, food safety and health cards while improving oversight and administration in Alberta’s health system.
If passed, Bill 11, the Health Statutes Amendment Act, 2025 (No. 2), would amend several pieces of legislation to reflect Alberta’s evolving health needs, strengthen the ability of health care professionals to deliver care and improve accountability and efficiency across the system.
“This legislation represents a new era for health care in Alberta. By putting patients first and supporting providers, we are improving transparency, flexibility and access. With modernized physician rules, stronger drug coverage, enhanced food safety and better health information sharing, Albertans will have world-class care.”
Protecting drug coverage for Albertans
If passed, amendments would improve coordination between public and private drug plans, ensuring taxpayer-funded programs are used efficiently and remain available for those who need them most.
Private plans would become the first payer for individuals who have them, with public programs acting as a safety net. The legislation would also protect older Albertans by ensuring employers cannot reduce or terminate health benefits for employees aged 65 and older who remain actively employed.
“People shouldn’t be punished for getting older – it’s that straightforward. With this legislation, we’re protecting Albertans by ensuring employers can no longer kick folks off their health benefits when they need them most.”
Ensuring consistent billing and remuneration practices
Alberta’s government is also proposing amendments to the Alberta Health Care Insurance Act to ensure health care providers and clinics are not engaging in improper billing practices and making inappropriate claims. The proposed amendments would strengthen accountability and transparency while generating cost savings by introducing penalties for systemic non-compliance.
Strengthening food safety in Alberta
If passed, amendments to the Public Health Act and related regulations would strengthen food safety across all establishments by improving training for staff, increasing transparency of inspection results and giving inspectors new tools for oversight and investigation.
The changes would also update the Food Regulation, Food Retail and Food Services Code, Institutions Regulation and create a new Public Health Investigator Regulation, ensuring consistent standards, better reporting and increased public confidence in Alberta’s food safety system.
“Enhancing food safety in Alberta is an important step to making sure Albertans have the safeguards and protections in place to keep them healthy and well. If passed, these amendments to the Public Health Act will ensure food establishments are following best practices and that enforcement measures are in place to support proper food safety.”
Improving health cards and information sharing
If passed, the legislation would create a new process for health card renewal, prevent card misuse and allow cards to be seized or suspended if tampered with. The changes would also permit information sharing with the ministries of Technology and Innovation and Service Alberta and Red Tape Reduction to support continued efforts to modernize health cards.
Amendments to the Health Information Act would support a more integrated health care system and seamless patient experience to help improve care for Albertans who are accessing the system.
It would also add new authority to enable health foundations to better connect with patients to support innovation and advancement of care in their community in an appropriate manner, in accordance with the requirements set out in regulations.
“Albertans generously support enhancements to health care delivery, innovation and research in their communities each year. We look forward to working with our health partners across the continuum to better communicate with grateful patients. With these changes, we will join other Canadian jurisdictions in connecting patients with health foundations in their community while ensuring the strongest protection of Albertans’ private health data.”
Advancing a new era of health care
If passed, proposed amendments to the Alberta Health Care Insurance Act and the Provincial Health Agencies Act would support operational changes to implement previously announced objectives like transitioning Alberta Health Services to a hospital-based acute care service provider.
The proposed amendments would also result in the repealing of the Hospitals Act, as all hospital governance and operational provisions would be moved into the Provincial Health Agencies Act.
New dual practice model to increase access and choice
The Health Statutes Amendment Act, 2025 (No. 2) includes proposed amendments to the Alberta Health Care Insurance Act that would modernize how physicians participate in Alberta’s publicly funded health insurance plan. The changes would introduce a new dual practice model, giving physicians greater flexibility to provide care in both public and private settings while maintaining safeguards to ensure Albertans continue to have access to publicly funded health services.

From LifeSiteNews
An NHS-backed trial will administer puberty blockers to children as young as 10 despite serious harms and is facing legal action from a prominent detransitioner.
Over 200 children in the United Kingdom will be injected with puberty blockers as part of an experiment on the effects of “gender transitioning.”
In November, King’s College London announced the Pathways Trial, which will track 226 gender-confused children as they take puberty blockers that are known to damage fertility, bone density, and brain development.
“Right now, there isn’t enough information about the possible benefits or risks that young people with gender incongruence may experience when taking puberty suppressing hormones,” a press release reads. “PATHWAYS TRIAL aims to help fill this gap in the evidence about what we know.”
READ: HHS study confirms dangers of transgender drugs, surgeries for minors
The Puberty Suppression and Transitional Healthcare with Adaptive Youth Services core trial, will administer puberty blockers to 226 children, from ages 10 to 15 years old, recruited over three years from the NHS.
The children will be divided into two groups and receive the drugs 12 months apart. After being given the drugs, the children will receive ongoing therapy, family counseling, and monitoring for two years.
Researchers claimed that the study has been “carefully checked by independent scientists” and is “overseen by two groups of people who are independent from the research team and the funders.”
Prominent detransitioner and outspoken activist Keira Bell condemned the experiment as a “betrayal of the children it claims to help” in a recent op-ed article published by The Telegraph.
“It will undoubtedly lead to infertility and lack of sexual function, to name only a couple,” she warned. “A child cannot fully understand these effects, let alone those that are unknown.”
On November 14, Bell, along with British psychotherapist James Esses, launched pre-action, demanding disclosure of trial documents. If the documents are not released, the pair promised to demand a judicial review.
📢 PRE-ACTION LETTERS SENT
Under instruction of @JamesEsses and I, legal have sent pre-action letters today to the regulatory bodies in charge of the puberty blocker trial.
They have been playing it sneaky, refusing to provide those important details to us since early this… pic.twitter.com/FVzAo2gVhO
— Keira Bell (@KBtheYoungOG) November 14, 2025
The research, approved and funded by the NHS, comes after puberty blockers were banned last year after a major review exposed the practice as dangerous and medically baseless.
The Cass Review is the world’s largest review into transgender interventions for minors. Dr. Hilary Cass, the pediatrician commissioned by the NHS to review the transgender “services” being made available to gender-confused minors, was scathing in her analysis.
Cass found that “gender medicine” is “built on shaky foundations” and that while these drastic interventions should be approached with extreme caution, “quite the reverse happened in the field of [so-called] gender care for children.”
LifeSiteNews has compiled a list of medical professions and experts who warn against “transgender” surgeries, warning of irreversible changes and lifelong side effects.
Moreover, internal documents from the World Professional Association for Transgender Health (WPATH) have shown that doctors who offer so-called “gender-affirming care” know that transgender hormones cause serious diseases, including cancer, but have prescribed them anyway.
The internal documents, dubbed the “WPATH FILES,” include emails and messages from a private discussion forum by doctors, as well as statements from a video call of WPATH members. The files reveal that the doctors working for WPATH know that so-called “gender-affirming care” can cause severe mental and physical disease and that it is impossible for minors to give “informed consent” to it.
As LifeSiteNews has previously noted, research does not support the assertions from transgender activists that surgical or pharmaceutical intervention to “affirm” confusion is “necessary medical care” or that it is helpful in preventing the suicides of gender-confused individuals.
In fact, in addition to asserting a false reality that one’s sex can be changed, transgender surgeries and drugs have been linked to permanent physical and psychological damage, including cardiovascular diseases, loss of bone density, cancer, strokes and blood clots, infertility, and suicidality.
There is also overwhelming evidence that those who undergo “gender transitioning” are more likely to commit suicide than those who are not given irreversible surgery. A Swedish study found that those who underwent “gender reassignment” surgery ended up with a 19.2 times greater risk of suicide.
Indeed, the most loving and helpful approach to people who think they are a different sex is not to validate them in their confusion but to show them the truth.
A study on the side effects of transgender “sex change” surgeries discovered that 81 percent of those who had undergone “sex change” surgeries in the past five years reported experiencing pain simply from normal movement in the weeks and months that followed — and that many other side effects manifest as well.


Psyop-Style Campaign That Delivered Mark Carney’s Win May Extend Into Floor-Crossing Gambits and Shape China–Canada–US–Mexico Relations

Expanding Canadian energy production could help lower global emissions

Trump Gives Zelenskyy Until Thanksgiving To Agree On Peace Deal, With U.S. Weapons And Intel On The Line

Bari Weiss Reportedly Planning To Blow Up Legacy Media Giant
-
 Health1 day ago
Health1 day agoTens of thousands are dying on waiting lists following decades of media reluctance to debate healthcare
-
 Alberta6 hours ago
Alberta6 hours agoPremier Smith explains how private clinics will be introduced in Alberta
-
 Opinion1 day ago
Opinion1 day agoLandmark 2025 Study Says Near-Death Experiences Can’t Be Explained Away
-
 Carbon Tax2 days ago
Carbon Tax2 days agoCarney fails to undo Trudeau’s devastating energy policies
-
 International2 days ago
International2 days agoCanada’s lost decade in foreign policy
-
 Business1 day ago
Business1 day agoBudget 2025: Ottawa Fakes a Pivot and Still Spends Like Trudeau
-
 armed forces2 days ago
armed forces2 days agoCanada At Risk Of Losing Control Of Its Northern Territories
-
 Business5 hours ago
Business5 hours agoUS Supreme Court may end ‘emergency’ tariffs, but that won’t stop the President