Addictions
A conversation with Premier Smith’s outgoing chief of staff, architect of Alberta’s recovery-focused drug policies

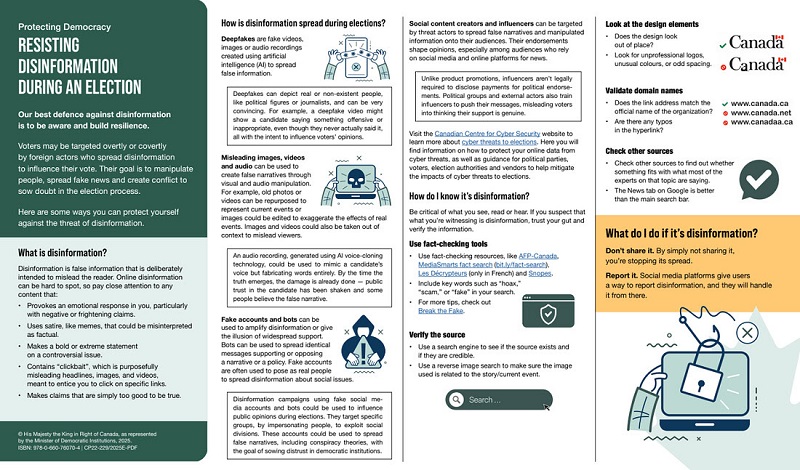
Marshall Smith, Alberta’s Chief of Staff, sits in his office at the Alberta Legislature in Edmonton

Marshall Smith, on what he has learned as an addict and policy leader and what’s next for him
Alberta Premier Danielle Smith’s chief of staff, Marshall Smith, is leaving his post at the end of October.
Since taking office in 2022, he has been instrumental in shaping Alberta’s drug policies and developing the Alberta Model — a recovery-focused addiction treatment policy that has gained international recognition for enhancing access to mental health and addiction services.
Under his guidance, Alberta has prioritized building recovery communities over harm-reduction programs. Government data show a 53 per cent decrease in opioid-related overdose deaths in June 2024 from the prior year, which may suggest Smith’s initiatives are having an impact.
In a statement on social media, the Premier shared that Smith informed her of his decision to retire earlier this year, after dedicating 32 years to public service. His departure comes just ahead of the United Conservative Party’s leadership review on Nov. 2.
Smith met with reporter Alexandra Keeler on Sept. 10 to discuss his personal journey from addiction to recovery and how it has shaped Alberta’s drug policies. On Oct. 10, they spoke by phone to discuss his recent decision to step down and what lies ahead for him.
AK: What emotional and psychological impact did your addiction have on your sense of self?
MS: It makes you feel powerless. Addiction is an illness of isolation, despair, loneliness and powerlessness. One of the hallmarks of addiction is continuing to use a substance despite a complete lack of control over your using, and over the circumstances that you’re in.
AK: Do you think that sense of powerlessness impacts an individual’s ability to provide informed consent for involuntary treatment?
MS: I think that, over time, if addiction is left unchecked or untreated, or is allowed to progress to its very latter stages, you absolutely lose agency over your ability to make decisions.
I used to get the question a lot: ‘Is it a disease? Is it a choice?’ And I say it’s both. It’s actually a disease of choices, which is to say that it’s a disease or an illness that affects my brain’s ability to make good choices.
AK: Were you the driving force behind Alberta’s shift away from harm reduction towards a recovery-focused approach, or was there a broader change in attitudes within the community?
MS: Certainly I’m not solely responsible. I’m a member of a broad community of people in recovery who have been advocating for these policies for two decades. I think that I have a background [and] certain skills that have found me in positions like this, where I can be most effective helping my community advance these ideas and concepts and actually get them implemented into policy and action.
AK: Obviously your lived experience with addiction brings a valuable perspective to the table. But what data sources are the province using to inform its addiction and recovery policies?
MS: We have a very broad literature base that we use to inform a lot of our policy decisions … Alberta [also] has the most comprehensive data collection and data analytics system in North America, bar none.
A practical example of how that’s useful is … [if] the data shows us that a very high number of people who were in custody — whether that’s corrections or police custody — went on to fatally overdose in a period after their release, that tells us that we need to focus on correctional programs, and we need to focus on policing programs.
And we’ve done that. We have amazing new correctional treatment programs that are second to none. I don’t know of anybody in Canada that’s doing this — we’ve taken [jail units where inmates sleep and live] and turned them into treatment centres, and connected them with our new treatment centres outside of jails. We partnered with police, because police have probably the most amount of contact with people who are using substances, and we gave them the ability to help people get on to opioid-substitution medications.
We’re going to go even further. Minister [of Mental Health and Addiction Dan] Williams has just announced the creation of the Centre of Recovery Excellence (CoRE), which is a first of its kind in Canada. It’s a Crown corporation not beholden to pharmaceutical money, which is a big change for us, and we were very deliberate about that.
[CoRE] will give us the ability to pull in data from across systems in government and have that data analyzed … So we’re entering into a very exciting time in terms of data and analytics around this issue.

AK: Without CoRE fully operational yet, what made you confident the recovery-focused approach would succeed?
MS: I see hundreds of thousands of Canadians every day entering recovery and maintaining their recovery … What I see in the alternative is a lot of drug use, homelessness, despair, disease [and] crime.
We spend a lot of time talking about data and evidence and science, and all of those things are good and necessary … but it’s not the only component of the decision-making process. … The policies that we’re making and the pathways that we take also have to be informed by the values of the community that we serve. … For far too long in Canada, that hasn’t been a consideration.
I think that we are at a place in Canada where the country is saying to us it’s time to revisit the direction that we’ve been going. I think that they’re saying to us, as policymakers, that we gave this a chance. We had become convinced by experts and the media … to give [pro-drug, harm-reduction policies like safer supply] a try …
[A]fter 20 years of that, I think that Canadians are ready to throw in the towel and to say, ‘We’re done with this. We’ve given you enough time to prove out your thesis. It’s not worked, and now we’re looking for fresh ideas.’
So Alberta is here leading that conversation of fresh and different ideas, and we’re happy to have that role.
The remainder of this interview took place on Oct. 10.
AK: Premier Smith announced your retirement at the end of October. What prompted your decision to step down?
MS: My time in Alberta has been a lengthy and intense role of system transformation over two premiers and standing up government twice.
While there’s still a lot of work to be done here, we have a tremendous team in Alberta that is leading that work under Minister Williams. I just felt that it’s time for me to step out of the role and continue to serve in other capacities.
AK: Looking ahead, what aspects of the Alberta Model will you carry with you into your future endeavours?
MS: I would say all aspects of the model need to be expanded across Canada, for jurisdictions that are interested.
Where I can be of the most assistance to other governments is talking to them about how to effectively organize themselves to be successful in this area. I think that governments across the country are struggling to figure out how to do that.
AK: What new opportunities do you hope to pursue that you haven’t been able to explore during your time in this role? Will your focus continue to be in addiction and drug policy?
MS: The majority of my focus will be on addiction and drug policy, but I have other areas of interest.
I’m passionate about the work that we’re doing with Indigenous people … I’m also very passionate about emerging technology and how we’re going to use that to uncover some of the answers that we’re looking for on these models.
I’m looking forward to having a little bit more freedom and focus.
This interview has been edited and condensed for clarity.
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.
Subscribe to Break The Needle. Our content is always free – but if you want to help us commission more high-quality journalism, consider getting a voluntary paid subscription.

2025 Federal Election
Poilievre to invest in recovery, cut off federal funding for opioids and defund drug dens

From Conservative Party Communications
Poilievre will Make Recovery a Reality for 50,000 Canadians
Conservative Leader Pierre Poilievre pledged he will bring the hope that our vulnerable Canadians need by expanding drug recovery programs, creating 50,000 new opportunities for Canadians seeking freedom from addiction. At the same time, he will stop federal funding for opioids, defund federal drug dens, and ensure that any remaining sites do not operate within 500 meters of schools, daycares, playgrounds, parks and seniors’ homes, and comply with strict new oversight rules that focus on pathways to treatment.
More than 50,000 people have lost their lives to fentanyl since 2015—more Canadians than died in the Second World War. Poilievre pledged to open a path to recovery while cracking down on the radical Liberal experiment with free access to illegal drugs that has made the crisis worse and brought disorder to local communities.
Specifically, Poilievre will:
- Fund treatment for 50,000 Canadians. A new Conservative government will fund treatment for 50,000 Canadians in treatment centres with a proven record of success at getting people off drugs. This includes successful models like the Bruce Oake Recovery Centre, which helps people recover and reunite with their families, communities, and culture. To ensure the best outcomes, funding will follow results. Where spaces in good treatment programs exist, we will use them, and where they need to expand, these funds will allow that.
- Ban drug dens from being located within 500 metres of schools, daycares, playgrounds, parks, and seniors’ homes and impose strict new oversight rules. Poilievre also pledged to crack down on the Liberals’ reckless experiments with free access to illegal drugs that allow provinces to operate drug sites with no oversight, while pausing any new federal exemptions until evidence justifies they support recovery. Existing federal sites will be required to operate away from residential communities and places where families and children frequent and will now also have to focus on connecting users with treatment, meet stricter regulatory standards or be shut down. He will also end the exemption for fly-by-night provincially-regulated sites.
“After the Lost Liberal Decade, Canada’s addiction crisis has spiralled out of control,” said Poilievre. “Families have been torn apart while children have to witness open drug use and walk through dangerous encampments to get to school. Canadians deserve better than the endless Liberal cycle of crime, despair, and death.”
Since the Liberals were first elected in 2015, our once-safe communities have become sordid and disordered, while more and more Canadians have been lost to the dangerous drugs the Liberals have flooded into our streets. In British Columbia, where the Liberals decriminalized dangerous drugs like fentanyl and meth, drug overdose deaths increased by 200 percent.
The Liberals also pursued a radical experiment of taxpayer-funded hard drugs, which are often diverted and resold to children and other vulnerable Canadians. The Vancouver Police Department has said that roughly half of all hydromorphone seizures were diverted from this hard drugs program, while the Waterloo Regional Police Service and Niagara Regional Police Service said that hydromorphone seizures had exploded by 1,090% and 1,577%, respectively.
Despite the death and despair that is now common on our streets, bizarrely Mark Carney told a room of Liberal supporters that 50,000 fentanyl deaths in Canada is not “a crisis.” He also hand-picked a Liberal candidate who said the Liberals “would be smart to lean into drug decriminalization” and another who said “legalizing all drugs would be good for Canada.”
Carney’s star candidate Gregor Robertson, an early advocate of decriminalization and so-called safe supply, wanted drug dens imposed on communities without any consultation or public safety considerations. During his disastrous tenure as Vancouver Mayor, overdoses increased by 600%.
Alberta has pioneered an approach that offers real hope by adopting a recovery-focused model of care, leading to a nearly 40 percent reduction in drug-poisoning deaths since 2023—three times the decrease seen in British Columbia. However, we must also end the Liberal drug policies that have worsened the crisis and harmed countless lives and families.
To fund this policy, a Conservative government will stop federal funding for opioids, defund federal drug dens, and sue the opioid manufacturers and consulting companies who created this crisis in the first place.
“Canadians deserve better than the Liberal cycle of crime, despair, and death,” said Poilievre. “We will treat addiction with compassion and accountability—not with more taxpayer-funded poison. We will turn hurt into hope by shutting down drug dens, restoring order in our communities, funding real recovery, and bringing our loved ones home drug-free.”

By Adam Zivo
Sweden, the U.K., and Canada all experimented with providing opioids to addicts. The results were disastrous.
[This article was originally published in City Journal, a public policy magazine and website published by the Manhattan Institute for Policy Research. We encourage our readers to subscribe to them for high-quality analysis on urban issues]
Last August, Denver’s city council passed a proclamation endorsing radical “harm reduction” strategies to address the drug crisis. Among these was “safer supply,” the idea that the government should give drug users their drug of choice, for free. Safer supply is a popular idea among drug-reform activists. But other countries have already tested this experiment and seen disastrous results, including more addiction, crime, and overdose deaths. It would be foolish to follow their example.
The safer-supply movement maintains that drug-related overdoses, infections, and deaths are driven by the unpredictability of the black market, where drugs are inconsistently dosed and often adulterated with other toxic substances. With ultra-potent opioids like fentanyl, even minor dosing errors can prove fatal. Drug contaminants, which dealers use to provide a stronger high at a lower cost, can be just as deadly and potentially disfiguring.
Because of this, harm-reduction activists sometimes argue that governments should provide a free supply of unadulterated, “safe” drugs to get users to abandon the dangerous street supply. Or they say that such drugs should be sold in a controlled manner, like alcohol or cannabis—an endorsement of partial or total drug legalization.
But “safe” is a relative term: the drugs championed by these activists include pharmaceutical-grade fentanyl, hydromorphone (an opioid as potent as heroin), and prescription meth. Though less risky than their illicit alternatives, these drugs are still profoundly dangerous.
The theory behind safer supply is not entirely unreasonable, but in every country that has tried it, implementation has led to increased suffering and addiction. In Europe, only Sweden and the U.K. have tested safer supply, both in the 1960s. The Swedish model gave more than 100 addicts nearly unlimited access through their doctors to prescriptions for morphine and amphetamines, with no expectations of supervised consumption. Recipients mostly sold their free drugs on the black market, often through a network of “satellite patients” (addicts who purchased prescribed drugs). This led to an explosion of addiction and public disorder.
Most doctors quickly abandoned the experiment, and it was shut down after just two years and several high-profile overdose deaths, including that of a 17-year-old girl. Media coverage portrayed safer supply as a generational medical scandal and noted that the British, after experiencing similar problems, also abandoned their experiment.
While the U.S. has never formally adopted a safer-supply policy, it experienced something functionally similar during the OxyContin crisis of the 2000s. At the time, access to the powerful opioid was virtually unrestricted in many parts of North America. Addicts turned to pharmacies for an easy fix and often sold or traded their extra pills for a quick buck. Unscrupulous “pill mills” handed out prescriptions like candy, flooding communities with OxyContin and similar narcotics. The result was a devastating opioid epidemic—one that rages to this day, at a cumulative cost of hundreds of thousands of American lives. Canada was similarly affected.
The OxyContin crisis explains why many experienced addiction experts were aghast when Canada greatly expanded access to safer supply in 2020, following a four-year pilot project. They worried that the mistakes of the recent past were being made all over again, and that the recently vanquished pill mills had returned under the cloak of “harm reduction.”
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Most Canadian safer-supply prescribers dispense large quantities of hydromorphone with little to no supervised consumption. Patients can receive up to 40 eight-milligram pills per day—despite the fact that just two or three are enough to cause an overdose in someone without opioid tolerance. Some prescribers also provide supplementary fentanyl, oxycodone, or stimulants.
Unfortunately, many safer-supply patients sell or trade a significant portion of these drugs—primarily hydromorphone—in order to purchase more potent illicit substances, such as street fentanyl.
The problems with safer supply entered Canada’s consciousness in mid-2023, through an investigative report I wrote for the National Post. I interviewed 14 addiction physicians from across the country, who testified that safer-supply diversion is ubiquitous; that the street price of hydromorphone collapsed by up to 95 percent in communities where safer supply is available; that youth are consuming and becoming addicted to diverted safer-supply drugs; and that organized crime traffics these drugs.
Facing pushback, I interviewed former drug users, who estimated that roughly 80 percent of the safer-supply drugs flowing through their social circles was getting diverted. I documented dozens of examples of safer-supply trafficking online, representing tens of thousands of pills. I spoke with youth who had developed addictions from diverted safer supply and adults who had purchased thousands of such pills.
After months of public queries, the police department of London, Ontario—where safer supply was first piloted—revealed last summer that annual hydromorphone seizures rose over 3,000 percent between 2019 and 2023. The department later held a press conference warning that gangs clearly traffic safer supply. The police departments of two nearby midsize cities also saw their post-2019 hydromorphone seizures increase more than 1,000 percent.
The Canadian government quietly dropped its support for safer supply last year, cutting funding for many of its pilot programs. The province of British Columbia (the nexus of the harm-reduction movement) finally pulled back support last month, after a leaked presentation confirmed that safer-supply drugs are getting sold internationally and that the government is investigating 60 pharmacies for paying kickbacks to safer-supply patients. For now, all safer-supply drugs dispensed within the province must be consumed under supervision.
Harm-reduction activists have insisted that no hard evidence exists of widespread diversion of safer-supply drugs, but this is only because they refuse to study the issue. Most “studies” supporting safer supply are produced by ideologically driven activist-scholars, who tend to interview a small number of program enrollees. These activists also reject attempts to track diversion as “stigmatizing.”
The experiences of Sweden, the United Kingdom, and Canada offer a clear warning: safer supply is a reliably harmful policy. The outcomes speak for themselves—rising addiction, diversion, and little evidence of long-term benefit.
As the debate unfolds in the United States, policymakers would do well to learn from these failures. Americans should not be made to endure the consequences of a policy already discredited abroad simply because progressive leaders choose to ignore the record. The question now is whether we will repeat others’ mistakes—or chart a more responsible course.
Our content is always free –
but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.


RCMP Whistleblowers Accuse Members of Mark Carney’s Inner Circle of Security Breaches and Surveillance

MEI-Ipsos poll: 56 per cent of Canadians support increasing access to non-governmental healthcare providers
AI-Driven Election Interference from China, Russia, and Iran Expected, Canadian Security Officials Warn

Trump Executive Orders ensure ‘Beautiful Clean’ Affordable Coal will continue to bolster US energy grid
-
Daily Caller2 days ago
Trump Executive Orders ensure ‘Beautiful Clean’ Affordable Coal will continue to bolster US energy grid
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoBREAKING from THE BUREAU: Pro-Beijing Group That Pushed Erin O’Toole’s Exit Warns Chinese Canadians to “Vote Carefully”
-
 Business2 days ago
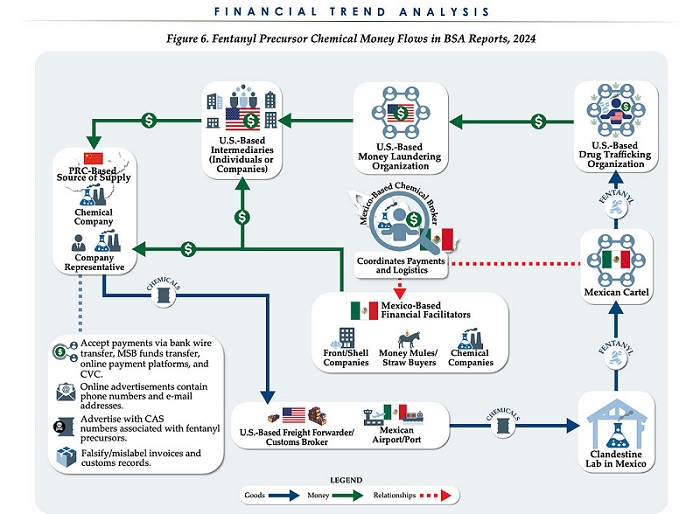
Business2 days agoChina, Mexico, Canada Flagged in $1.4 Billion Fentanyl Trade by U.S. Financial Watchdog
-
 COVID-191 day ago
COVID-191 day agoTamara Lich and Chris Barber trial update: The Longest Mischief Trial of All Time continues..
-
 Energy2 days ago
Energy2 days agoStraits of Mackinac Tunnel for Line 5 Pipeline to get “accelerated review”: US Army Corps of Engineers
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoAllegations of ethical misconduct by the Prime Minister and Government of Canada during the current federal election campaign
-
 2025 Federal Election16 hours ago
2025 Federal Election16 hours agoPRC-Linked Disinformation Claims Conservatives Threaten Chinese Diaspora Interests, Take Aim at PM Carney’s Debate Remark
-
 Daily Caller2 days ago
Daily Caller2 days agoDOJ Releases Dossier Of Deported Maryland Man’s Alleged MS-13 Gang Ties