Alberta
ASIRT rules police officer’s use of lethal force permissible in this case


From the Alberta Serious Incident Response Team (ASIRT)
Edmonton officer acted reasonably in fatal shooting
On March 9, 2017, the Alberta Serious Incident Response Team (ASIRT) was directed to investigate the circumstances surrounding an Edmonton Police Service (EPS) officer-involved shooting that occurred the same day that resulted in the death of a 55-year-old man.
Shortly before 1:30 p.m., multiple 911 calls were made regarding a possible impaired motorist driving a minivan on 149 Street that had entered onto the Whitemud Freeway. The make, model, and vehicle’s licence plate number were provided to police. Two independent callers to police both described the driver, who was the lone occupant of the van, indicating that he looked “drunk.” Police were advised that the van had earlier hit a snowbank and a curb, was being driven in and out of lanes, “swerving all over the road,” including down the middle of two lanes and had nearly collided with a vehicle. The van was reportedly “all over the road” and at one point, went off the roadway. As the van approached the 119 Street exit, it almost collided with another vehicle, and both callers advised that other vehicles were “swerving” to avoid the van. One of the callers advised police that the van was driving at speeds between 30 and 120 km/h. The driver took the freeway exit ramp southbound on 119 Street, followed by one of the callers.
As the driver went south on 119 Street, swerving along the way, he turned right at 23 Avenue to proceed westbound, driving close to and over the curb, and nearly colliding with concrete blocks on a small bridge over a ravine. It was reported that the van looked like it was about to crash. After turning onto Hodgson Way, driving over the curb along the way, the driver turned into a cul-de-sac, stopped in the middle of the road, then returned to Hodgson Way at a higher speed. The driver then turned into Holland Landing, at which point a marked EPS vehicle pulled up, so the caller who was following the van went on his way, leaving the driver to the police. He did not observe any interaction between police and the driver of the vehicle.
The lone EPS officer, in full uniform, had arrived on scene in a marked police SUV. He observed the van, matching the earlier provided description, coming directly towards him, driven by a large man, also matching the description provided. The van stopped and the officer pulled the front end of the police SUV up to the front end of the van, slightly to the driver’s side to block the vehicle.
The officer exited his vehicle and approached the van. As he did so, the man exited the van against the officer’s commands to remain in the vehicle. The officer noted signs of the man’s impairment including the smell of liquor, glazed eyes, difficulty focusing, and swaying from side to side. When questioned, the man said he had not been drinking, but slurred his words. The officer told the man he was under arrest for impaired driving, and ordered him to turn around and place his hands behind his back. The man asked, “what do you want me to do?”, and the command was repeated. When the officer tried to take control of the man’s arm, the man went to reach for something at his waist. The officer instructed the man to keep his hands visible, and stepped back to call for assistance. This call took place approximately 50 seconds after the initial traffic stop.
The officer again instructed the man to show his hands. At this point, the man produced a hunting knife in his right hand. The man was described as raising the knife in front of his body and pointing it at the officer. The officer attempted to gain distance but the man followed the officer. The officer slipped on the roadway, covered in fresh snow, and fell to his back. As he tried to get up, the man fell on top of him, still holding the knife in his right hand. The officer yelled several commands for the man to “stop” and “get back”, and tried to push him away. The officer kicked the man away to gain space, and continued to shout commands to drop the weapon and “get back”. When the man again advanced, still holding the knife, the officer discharged four rounds from his service pistol from his position on the ground. He saw the man fall away to the left. The officer rose to his feet, and called in “shots fired” stating “he came at me with a knife”. This second call was approximately 20 seconds after the first call for assistance.
The situation between the officer and the man had deteriorated extremely quickly. The time between when the officer indicated that he was “off” with the subject, meaning he was going to go deal with him, and the time that he reported shots had been fired was one minute, 14 seconds.
The knife was still in the right hand of the man, who had fallen on the snow-covered roadway. The officer holstered his firearm, moved the knife away from the man and attempted CPR until other officers arrived on scene.

No civilian witnesses saw the actual shooting, but several were present and made observations immediately after the shots were fired. Upon hearing the shots, two witnesses exited their residence. One of these witnesses reported that just prior to hearing the shots fired, he heard yelling but could not hear what was being said. The officer was described as breathing heavily, had snow on his face and in his hair, and was described as looking like he had been in “a battle”. A photograph that was taken at the time by one of the witnesses showed snow on the back of the officer’s patrol jacket and pants. Another civilian witness reported he heard shots, looked out his front window and saw a man lying on the street and a uniformed police officer standing within a foot of the person. He advised investigators that he watched the police officer holster his sidearm, walk towards the man, remove a knife from the man’s hand to move it approximately three feet from the body towards the sidewalk.
The knife recovered from the scene matched the branded sheath found attached to the man’s belt. A DNA profile from the handle of the knife matched the DNA profile of the man. The man was also known to carry a hunting knife. The man was 55 years of age at the time of his death. He held dual Russian and Canadian citizenship. He had been an Edmonton resident for years and operated his own business and worked as a sub-contractor. He was not working on March 9, 2017 because of inclement weather. He has no prior criminal record. By all accounts, the man’s conduct with the officer on March 9, 2017 was out of character.
Upon autopsy, the man’s blood alcohol level was determined to be at least three and a half times over the legal limit of 80 mg/%.
As established by the high blood alcohol results, the egregious driving pattern observed by civilians, the observations of the civilian witnesses and the officer as to the physical signs of impairment, the man was grossly intoxicated at the time of his death. This level of intoxication would not only have resulted in physical signs of impairment but would also have compromised thought processes, judgment, perception and a person’s intellectual and emotional functioning.
Under the Criminal Code, a police officer is authorized to use as much force as is reasonably necessary to perform his or her lawful duties. This can include force intended, or likely to cause, death or grievous bodily harm if the officer reasonably believes that such force is necessary to defend themselves or someone under their protection from imminent death or grievous bodily harm. Further, any person, including a police officer, is entitled to use reasonable force in self-defence or in defence of another person. An assessment of the reasonableness of force will consider different factors, including the use (or threatened use) of a weapon, the imminence of the threat, other options available and the nature of the force (or threat of force) itself.
The officer had more than reasonable grounds to believe that the man was operating a motor vehicle while his ability to do so was impaired by alcohol. He was lawfully placed and acting in the lawful execution of his duty, and had both the grounds and the authority to place the man under arrest.
Based on the available evidence as a whole, it is very clear that the conduct of the man presented a very real risk of death to the officer. The situation escalated at the point when the man twisted away and produced the knife. In response to these actions, the officer attempted to reposition himself to reduce the threat, and had issued numerous commands to the man to stop and to drop the weapon. The man was non-compliant with those commands, and initiated a physical confrontation with the officer, despite the officer’s attempts to create distance, and did so while armed with a knife. In the circumstances, the officer’s conduct was clearly objectively and subjectively reasonable and necessary. When assessing the danger posed to the officer by the man, and factors such as the presence of a weapon, the immediacy of the threat to the officer, and the lack of time, distance or the availability of other alternatives, it is evident that the action taken by the subject officer, while tragic, was reasonable in the circumstances. As such, the subject officer’s use of lethal force, having regard to the protections provided in the Criminal Code, was permissible and did not constitute a criminal offence.
ASIRT’s mandate is to effectively, independently, and objectively investigate incidents involving Alberta’s police that have resulted in serious injury or death to any person. This mandate includes incidents involving discharge of a firearm that would likely have resulted in serious injury or death had the person been struck.

From the Fraser Institute
By Nadeem Esmail, Mackenzie Moir and Lauren Asaad
In October, Alberta’s provincial government announced forthcoming legislative changes that will allow patients to pay out-of-pocket for any diagnostic test they want, and without a physician referral. The policy, according to the Smith government, is designed to help improve the availability of preventative care and increase testing capacity by attracting additional private sector investment in diagnostic technology and facilities.
Unsurprisingly, the policy has attracted Ottawa’s attention, with discussions now taking place around the details of the proposed changes and whether this proposal is deemed to be in line with the Canada Health Act (CHA) and the federal government’s interpretations. A determination that it is not, will have both political consequences by being labeled “non-compliant” and financial consequences for the province through reductions to its Canada Health Transfer (CHT) in coming years.
This raises an interesting question: While the ultimate decision rests with Ottawa, does the Smith government’s new policy comply with the literal text of the CHA and the revised rules released in written federal interpretations?
According to the CHA, when a patient pays out of pocket for a medically necessary and insured physician or hospital (including diagnostic procedures) service, the federal health minister shall reduce the CHT on a dollar-for-dollar basis matching the amount charged to patients. In 2018, Ottawa introduced the Diagnostic Services Policy (DSP), which clarified that the insured status of a diagnostic service does not change when it’s offered inside a private clinic as opposed to a hospital. As a result, any levying of patient charges for medically necessary diagnostic tests are considered a violation of the CHA.
Ottawa has been no slouch in wielding this new policy, deducting some $76.5 million from transfers to seven provinces in 2023 and another $72.4 million in 2024. Deductions for Alberta, based on Health Canada’s estimates of patient charges, totaled some $34 million over those two years.
Alberta has been paid back some of those dollars under the new Reimbursement Program introduced in 2018, which created a pathway for provinces to be paid back some or all of the transfers previously withheld on a dollar-for-dollar basis by Ottawa for CHA infractions. The Reimbursement Program requires provinces to resolve the circumstances which led to patient charges for medically necessary services, including filing a Reimbursement Action Plan for doing so developed in concert with Health Canada. In total, Alberta was reimbursed $20.5 million after Health Canada determined the provincial government had “successfully” implemented elements of its approved plan.
Perhaps in response to the risk of further deductions, or taking a lesson from the Reimbursement Action Plan accepted by Health Canada, the province has gone out of its way to make clear that these new privately funded scans will be self-referred, that any patient paying for tests privately will be reimbursed if that test reveals a serious or life-threatening condition, and that physician referred tests will continue to be provided within the public system and be given priority in both public and private facilities.
Indeed, the provincial government has stated they do not expect to lose additional federal health care transfers under this new policy, based on their success in arguing back previous deductions.
This is where language matters: Health Canada in their latest CHA annual report specifically states the “medical necessity” of any diagnostic test is “determined when a patient receives a referral or requisition from a medical practitioner.” According to the logic of Ottawa’s own stated policy, an unreferred test should, in theory, be no longer considered one that is medically necessary or needs to be insured and thus could be paid for privately.
It would appear then that allowing private purchase of services not referred by physicians does pass the written standard for CHA compliance, including compliance with the latest federal interpretation for diagnostic services.
But of course, there is no actual certainty here. The federal government of the day maintains sole and final authority for interpretation of the CHA and is free to revise and adjust interpretations at any time it sees fit in response to provincial health policy innovations. So while the letter of the CHA appears to have been met, there is still a very real possibility that Alberta will be found to have violated the Act and its interpretations regardless.
In the end, no one really knows with any certainty if a policy change will be deemed by Ottawa to run afoul of the CHA. On the one hand, the provincial government seems to have set the rules around private purchase deliberately and narrowly to avoid a clear violation of federal requirements as they are currently written. On the other hand, Health Canada’s attention has been aroused and they are now “engaging” with officials from Alberta to “better understand” the new policy, leaving open the possibility that the rules of the game may change once again. And even then, a decision that the policy is permissible today is not permanent and can be reversed by the federal government tomorrow if its interpretive whims shift again.
The sad reality of the provincial-federal health-care relationship in Canada is that it has no fixed rules. Indeed, it may be pointless to ask whether a policy will be CHA compliant before Ottawa decides whether or not it is. But it can be said, at least for now, that the Smith government’s new privately paid diagnostic testing policy appears to have met the currently written standard for CHA compliance.

Nadeem Esmail

Mackenzie Moir

Lauren Asaad
Policy Analyst, Fraser Institute

From the Fraser Institute
By Tegan Hill and Austin Thompson
In cities across the country, modest homes have become unaffordable for typical families. Calgary and Edmonton have not been immune to this trend, but they’ve weathered it better than most—largely by making it easier to build homes.
Specifically, faster permit approvals, lower municipal fees and fewer restrictions on homebuilders have helped both cities maintain an affordability edge in an era of runaway prices. To preserve that edge, they must stick with—and strengthen—their pro-growth approach.
First, the bad news. Buying a home remains a formidable challenge for many families in Calgary and Edmonton.
For example, in 2023 (the latest year of available data), a typical family earning the local median after-tax income—$73,420 in Calgary and $70,650 in Edmonton—had to save the equivalent of 17.5 months of income in Calgary ($107,300) or 12.5 months in Edmonton ($73,820) for a 20 per cent down payment on a typical home (single-detached house, semi-detached unit or condominium).
Even after managing such a substantial down payment, the financial strain would continue. Mortgage payments on the remaining 80 per cent of the home’s price would have required a large—and financially risky—share of the family’s after-tax income: 45.1 per cent in Calgary (about $2,757 per month) and 32.2 per cent in Edmonton (about $1,897 per month).
Clearly, unless the typical family already owns property or receives help from family, buying a typical home is extremely challenging. And yet, housing in Calgary and Edmonton remains far more affordable than in most other Canadian cities.
In 2023, out of 36 major Canadian cities, Edmonton and Calgary ranked 8th and 14th, respectively, for housing affordability (relative to the median after-tax family income). That’s a marked improvement from a decade earlier in 2014 when Edmonton ranked 20th and Calgary ranked 30th. And from 2014 to 2023, Edmonton was one of only four Canadian cities where median after-tax family income grew faster than the price of a typical home (in Calgary, home prices rose faster than incomes but by much less than in most Canadian cities). As a result, in 2023 typical homes in Edmonton cost about half as much (again, relative to the local median after-tax family income) as in mid-sized cities such as Windsor and Kelowna—and roughly one-third as much as in Toronto and Vancouver.
To be clear, much of Calgary and Edmonton’s improved rank in affordability is due to other cities becoming less and less affordable. Indeed, mortgage payments (as a share of local after-tax median income) also increased since 2014 in both Calgary and Edmonton.
But the relative success of Alberta’s two largest cities shows what’s possible when you prioritize homebuilding. Their approach—lower municipal fees, faster permit approvals and fewer building restrictions—has made it easier to build homes and helped contain costs for homebuyers. In fact, homebuilding has been accelerating in Calgary and Edmonton, in contrast to a sharp contraction in Vancouver and Toronto. That’s a boon to Albertans who’ve been spared the worst excesses of the national housing crisis. It’s also a demographic and economic boost for the province as residents from across Canada move to Alberta to take advantage of the housing market—in stark contrast to the experience of British Columbia and Ontario, which are hemorrhaging residents.
Alberta’s big cities have shown that when governments let homebuilders build, families benefit. To keep that advantage, policymakers in Calgary and Edmonton must stay the course.

Tegan Hill
Director, Alberta Policy, Fraser Institute

Austin Thompson
Senior Policy Analyst, Fraser Institute


Politicians should be honest about environmental pros and cons of electric vehicles

Canada releases new digital ID app for personal documents despite privacy concerns

Charitable giving on the decline in Canada
NFL Ice Bowls Turn Down The Thermostat on Climate Change Hysteria
-
Automotive16 hours ago
Politicians should be honest about environmental pros and cons of electric vehicles
-
 Daily Caller2 days ago
Daily Caller2 days ago‘Almost Sounds Made Up’: Jeffrey Epstein Was Bill Clinton Plus-One At Moroccan King’s Wedding, Per Report
-
 Crime2 days ago
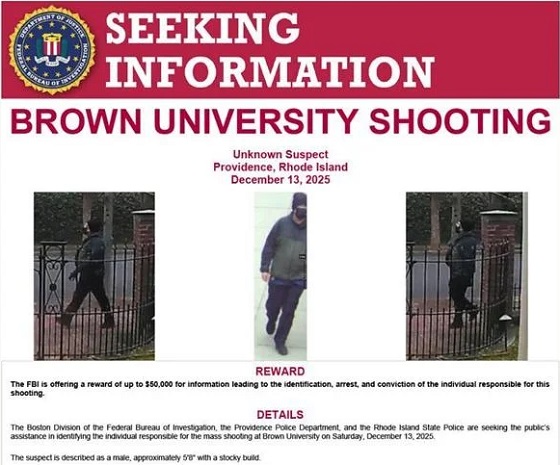
Crime2 days agoBrown University shooter dead of apparent self-inflicted gunshot wound
-
 Business2 days ago
Business2 days agoTrump signs order reclassifying marijuana as Schedule III drug
-
 Bruce Dowbiggin1 day ago
Bruce Dowbiggin1 day agoHunting Poilievre Covers For Upcoming Demographic Collapse After Boomers
-
Alberta1 day ago
Alberta’s new diagnostic policy appears to meet standard for Canada Health Act compliance
-
Alberta2 days ago
Housing in Calgary and Edmonton remains expensive but more affordable than other cities
-
 Censorship Industrial Complex1 day ago
Censorship Industrial Complex1 day agoTop constitutional lawyer warns against Liberal bills that could turn Canada into ‘police state’