Health
As cancer rates soar in younger people, experts seek answers

From LifeSiteNews
By John-Michael Dumais, The Defender
Two recent reports by the American Cancer Society reveal alarming increases in numerous cancers among millennials and Gen Z in the U.S. While mainstream medical experts debate causes, some doctors told The Defender mRNA vaccines may be to blame for the recent emergence of aggressive cancers that often don’t respond to conventional treatments.
Cancer rates among younger generations are rising at an alarming pace, with medical professionals reporting unprecedented increases in aggressive cancers over the past few years.
A study published in the August edition of The Lancet Public Health revealed that through 2019, the incidence rates for 17 of 34 cancer types were increasing in progressively younger people in the U.S., ABC News reported on July 31.
Lead author Ahmedin Jemal, DVM, Ph.D., from the American Cancer Society (ACS) told The Washington Post that if current trends in cancer and mortality rates among Gen X and millennials continue, it “may halt or even reverse the progress that we have made in reducing cancer mortality over the past several decades.”
More recent data from the ACS’ “Cancer statistics, 2024” report — with data on cancer incidence through 2020 and mortality through 2021 — showed the trend continuing.
As of 2021, among adults under 50, colorectal cancer has become the leading cause of cancer death in men and the second-leading cause in women, despite ranking fourth for both sexes in the late 1990s.
Some researchers point to lifestyle, poverty and environmental factors as potential causes for the uptick in cancers, while others suggest the COVID-19 mRNA vaccines may be to blame for the rise in “turbo cancers.”
Meanwhile, Pfizer in December 2023 spent $43 billion for Seagan, a “cancer care” biotech company with only $2.2 billion in sales. Seagan’s already-approved drugs include those for bladder cancer, cervical cancer, breast cancer and Hodgkin lymphoma.
The acquisition expands Pfizer’s oncology portfolio to 25 approved drugs, which, by the second quarter of this year, helped the company recover from last year’s drop in COVID-19 vaccine sales when its stock lost half its value.
The cancer trend has also caught the attention of health organizations worldwide, including the World Health Organization, which in February predicted a 77% rise in new cancer cases — from 20 million cases in 2022 to over 35 million cases by 2050.
Which cancers are on the rise?
The Lancet study revealed disturbing trends in cancer rates for people born between 1920 and 1990, finding that through 2019, incidence rates for 17 of 34 cancer types analyzed were increasing in progressively younger birth cohorts.
For some cancers, the incidence rate was approximately 1 to 3 times higher in the 1990 birth cohort (people in their late 20s at the time of the study) compared to the 1955 birth cohort (people in their mid-60s at the time of the study).
Particularly concerning were the increases in cancers of the small intestine (256% higher), kidney and renal pelvis (192% higher), and pancreas in both males and females (161% higher). For women, liver and intrahepatic bile duct cancer rates also saw a significant uptick (105% higher).
In younger cohorts, cancer incidence also increased for estrogen receptor-positive breast cancer, uterine corpus (endometrial) cancer, colorectal cancer, non-cardia gastric (stomach) cancer, gallbladder and other biliary cancer, ovarian cancer, and testicular cancer, anal cancer and Kaposi sarcoma in males.
For those around 30 years old, cancer rates increased an average of 12% across all cancer types.
The study also noted that mortality rates mirrored incidence trends for several cancers, including liver cancer in females, uterine corpus, gallbladder and other biliary, testicular and colorectal cancers. This suggests that the increase in incidence is substantial enough to outweigh improvements in cancer survival rates.
The findings from the ACS’ cancer statistics report, which contains data through 2021, provide additional context to the rising cancer rates in younger generations, particularly for colorectal cancer in both sexes and breast, cervical, uterine and liver cancers in women.
The Ethical Skeptic, a well-regarded statistician on the social platform X, posted more recent cancer mortality data. The following graph, based on the Centers for Disease Control and Prevention’s WONDER online databases, shows excess mortality from malignant neoplasms (spreading tumors) “elevated 29% and still rising” for ages 0-54 through week 22 of 2024:

More recent ‘turbo cancers’
Dr. William Makis, a Canadian board-certified nuclear medicine radiologist and oncologist, reported in an interview on the “America Out Loud PULSE” podcast on July 6 that he has seen “just an explosion of extremely aggressive cancers in very young individuals” since the COVID-19 pandemic began.
Cancers Makis identified that are particularly affecting younger populations include breast cancer, colon cancer, bile duct cancer, pancreatic cancer, leukemia and lymphoma.
Makis emphasized that these cancers are presenting at advanced stages (3 or 4), are behaving “very aggressively” and are often resistant to conventional treatments. He referred to these as “turbo cancers” due to their rapid growth and spread.
Emmy Award winning FOX 4 Morning Reporter Matt Stewart announces he has Cancer – His Wife has also developed Cancer – 💔
“Friends, I have some devastating news to share with all of you. I have been feeling a little off mentally lately – dizzy, nauseous, a little double vision.… pic.twitter.com/NaiVzj8qN1
— “Sudden And Unexpected” (@toobaffled) July 28, 2024
Dr. Angus Dalgleish, a renowned oncologist and professor at St. George’s, University of London, has reported rapidly progressing cancers in patients receiving COVID-19 mRNA booster shots, although he did not specify the ages affected.
In particular, melanoma patients who had been in remission in his practice experienced sudden relapses. Cancer doctors around the world told him him about rapidly accelerating cancers, including lymphomas, leukemia, kidney and colorectal cancer and “multiple metastatic spread” of cancers throughout the body.
A Japanese study published in April in the journal Cureus reported post-COVID-19-vaccination increases in mortality for most age groups, including those under 50 years old. Cancers with the highest excess mortality rates included ovarian cancer, leukemia, prostate cancer, lip/oral/pharyngeal cancer and pancreatic cancer.

We do not have the data to point to
Mainstream medical experts have proposed several theories to explain the rising cancer rates among younger generations.
In the Lancet paper, the authors attribute the increase in cancers in younger people to higher exposure to carcinogens early in life, obesity, unhealthy diet, environmental chemicals, changes in reproductive patterns and alcohol-related behaviors.
In its “Cancer statistics, 2024” report, the ACS pointed to several additional potential culprits, including poverty-related factors such as inadequate health insurance and lack of access to screening and high-quality healthcare, and to structural racism-related factors, including mortgage lending bias and neighborhood-level redlining.
Dr. William Dahut, a medical oncologist and ACS chief scientific officer, told ABC News that finding a single cause is difficult. “It’s so easy for us to say ‘yes, it’s obesity’; ‘yes, it’s lack of exercise’; ‘yes, it’s processed food.’ But we do not have the data to point to.”
Dr. Kevin Nead, a radiation oncologist and assistant professor in the Department of Epidemiology at the MD Anderson Cancer Center, told ABC News that something different could be happening with the biology of cancer in younger patients, indicating a need for new approaches to screening and early detection.
Left entirely unaddressed by the current mainstream medical and media reporting is the potential contribution to the rising rates of brain, thyroid and salivary gland cancers of EMR (electromagnetic radiation) exposure from cellphones, Bluetooth headsets, Wi-Fi routers and 4G/5G transmission towers.
Rapid cancer onset ‘basically impossible along the known paradigm’
Dr. Harvey Risch, professor emeritus of epidemiology at the Yale School of Public Health, told The Defender, “Clinicians have been seeing very strange things, for example, 25-year-olds with colon cancer who don’t have family histories of the disease.”
He stressed that this cancer typically takes decades to develop and that its appearance in younger people is “basically impossible along the known paradigm for how colon cancer works.”
On the podcast with Makis, Dr. Peter McCullough, a prominent cardiologist and researcher, also noted the typically longer lead time for cancers to develop.
“Is what we’re seeing now — are these just individuals who have cancers at the time they take the COVID vaccines or are these brand new cancers caused by the vaccines?” he asked.
Possible mechanisms for mRNA vaccine-caused cancers
Makis hypothesized that the mRNA vaccines could be accelerating already existing cancers and are likely responsible for the recent rise in aggressive cancers.
“These lipid nanoparticles [LNPs] — one of the key features is that they don’t stay in the arm. They end up in the systemic circulation,” Makis said.
He suggested that about 75% of the injection ends up in the bloodstream within a few hours, potentially depositing “pseudouridine, modified mRNA and DNA” throughout the body. He listed the brain, bone marrow, liver, pancreas, gall bladder, spleen, testes, ovaries, liver, colon and breast milk as among the locations where these components have been found.
“We are seeing cancers where there is deposition of these vaccine particles,” he said, noting that bone marrow deposition could be causing the increased incidence of leukemia.
Risch, while cautioning that long-term data is still lacking, pointed out potential mechanisms by which vaccines might affect cancer risk.
“The spike protein is toxic,” he stated. “The LNP itself is toxic. The biological manufacturing process involving inadequate filtration of possible harmful components can be toxic.”
Both Makis and Risch discussed the “IgG4 [immunoglobin type 4] antibody shift” caused by the mRNA vaccines as a likely contributor to rapid-onset cancers.
Risch explained how this particular antibody differs from IgG1 and IgG2 responses, which work to neutralize foreign pathogens. By contrast, IgG4 creates a “tolerance response” to keep the immune system from overreacting to things like pollen and food allergens.
Makis explained how after multiple mRNA injections, the level of IgG4 antibodies markedly increases, reducing immune surveillance, thus making “cancer invisible to your immune system.”
“If you’ve got tolerance to cancer cells, it’s not going to stop the cancer cells from reproducing,” Risch said. “You don’t want that to happen.”
Risch said that no one yet knows the depth of damage to the immune surveillance mechanisms the mRNA vaccines are causing, “but there are plausible mechanisms to be looking at.”
Full vid: https://t.co/76kyipSw0T
— Sense Receptor (@SenseReceptor) August 11, 2024


First responders say it is not overdoses that leave them feeling burned out—it is the endless cycle of calls they cannot meaningfully resolve
The soap bottle just missed his head.
Standing in the doorway of a cluttered Halifax apartment, Derek, a primary care paramedic, watched it smash against the wall.
Derek was there because the woman who threw it had called 911 again — she did so nearly every day. She said she had chest pain. But when she saw the green patch on his uniform, she erupted. Green meant he could not give her what she wanted: fentanyl.
She screamed at him to call “the red tags” — advanced care paramedics authorized to administer opioids. With none available, Derek declared the scene unsafe and left. Later that night, she called again. This time, a red-patched unit was available. She got her dose.
Derek says he was not angry at the woman, but at the system that left her trapped in addiction — and him powerless to help.
First responders across Canada say it is not overdoses that leave them feeling burned out — it is the endless cycle of calls they cannot meaningfully resolve. Understaffed, overburdened and dispatched into crises they are not equipped to fix, many feel morally and emotionally drained.
“We’re sending our first responders to try and manage what should otherwise be dealt with at structural and systemic levels,” said Nicholas Carleton, a University of Regina researcher who studies the mental health of public safety personnel.
Canadian Affairs agreed to use pseudonyms for the two frontline workers referenced in this story. Canadian Affairs also spoke with nine other first responders who agreed to speak only on background. All of these sources cited concerns about workplace retaliation for speaking out.
Moral injury
Canada’s opioid crisis is pushing frontline workers such as paramedics to the brink.
A 2024 study of 350 Quebec paramedics shows one in three have seriously considered suicide. Globally, ambulance workers have among the highest suicide rates of public service personnel.
Between 2017 and 2024, Canadian paramedics responded to nearly 240,000 suspected opioid overdoses. More than 50,000 of those were fatal.
Yet many paramedics say overdose calls are not the hardest part of the job.
“When they do come up, they’re pretty easy calls,” said Derek. Naloxone, a drug that reverses overdoses, is readily available. “I can actually fix the problem,” he said. “[It’s a] bit of instant gratification, honestly.”
What drains him are the calls they cannot fix: mental health crises, child neglect and abuse, homelessness.
“The ER has a [cardiac catheterization] lab that can do surgery in minutes to fix a heart attack. But there’s nowhere I can bring the mental health patients.
“So they call. And they call. And they call.”
Thomas, a primary care paramedic in Eastern Ontario, echoes that frustration.
“The ER isn’t a good place to treat addiction,” he said. “They need intensive, long-term psychological inpatient treatment and a healthy environment and support system — first responders cannot offer that.”
That powerlessness erodes trust. Paramedics say patients with addictions often become aggressive, or stop seeking help altogether.
“We have a terrible relationship with the people in our community struggling with addiction,” Thomas said. “They know they will sit in an ER bed for a few hours while being in withdrawals and then be discharged with a waitlist or no follow-up.”
Carleton, of the University of Regina, says that reviving people repeatedly without improvement decreases morale.
“You’re resuscitating someone time and time again,” said Carleton, who is also director of the Psychological Trauma and Stress Systems Lab, a federal unit dedicated to mental health research for public safety personnel. “That can lead to compassion fatigue … and moral injury.”
Katy Kamkar, a clinical psychologist focused on first responder mental health, says moral injury arises when workers are trapped in ethically impossible situations — saving a life while knowing that person will be back in the same state tomorrow.
“Burnout is … emotional exhaustion, depersonalization, and reduced personal accomplishment,” she said in an emailed statement. “High call volumes, lack of support or follow-up care for patients, and/or bureaucratic constraints … can increase the risk of reduced empathy, absenteeism and increased turnover.”
Kamkar says moral injury affects all branches of public safety, not just paramedics. Firefighters, who are often the first to arrive on the scene, face trauma from overdose deaths. Police report distress enforcing laws that criminalize suffering.
Understaffed and overburdened
Staffing shortages are another major stressor.
“First responders were amazing during the pandemic, but it also caused a lot of fatigue, and a lot of people left our business because of stress and violence,” said Marc-André Périard, vice president of the Paramedic Chiefs of Canada.
Nearly half of emergency medical services workers experience daily “Code Blacks,” where there are no ambulances available. Vacancy rates are climbing across emergency services. The federal government predicts paramedic shortages will persist over the coming decade, alongside moderate shortages of police and firefighters.
Unsafe work conditions are another concern. Responders enter chaotic scenes where bystanders — often fellow drug users — mistake them for police. Paramedics can face hostility from patients they just saved, says Périard.
“People are upset that they’ve been taken out of their high [when Naloxone is administered] and not realizing how close to dying they were,” he said.
Thomas says safety is undermined by vague, inconsistently enforced policies. And efforts to collect meaningful data can be hampered by a work culture that punishes reporting workplace dangers.
“If you report violence, it can come back to haunt you in performance reviews” he said.
Some hesitate to wait for police before entering volatile scenes, fearing delayed response times.
“[What] would help mitigate violence is to have management support their staff directly in … waiting for police before arriving at the scene, support paramedics in leaving an unsafe scene … and for police and the Crown to pursue cases of violence against health-care workers,” Thomas said.
“Right now, the onus is on us … [but once you enter], leaving a scene is considered patient abandonment,” he said.
Upstream solutions
Carleton says paramedics’ ability to refer patients to addiction and mental health referral networks varies widely based on their location. These networks rely on inconsistent local staffing, creating a patchwork system where people easily fall through the cracks.
“[Any] referral system butts up really quickly against the challenges our health-care system is facing,” he said. “Those infrastructures simply don’t exist at the size and scale that we need.”
Périard agrees. “There’s a lot of investment in safe injection sites, but not as much [resources] put into help[ing] these people deal with their addictions,” he said.
Until that changes, the cycle will continue.
On May 8, Alberta renewed a $1.5 million grant to support first responders’ mental health. Carleton welcomes the funding, but says it risks being futile without also addressing understaffing, excessive workloads and unsafe conditions.
“I applaud Alberta’s investment. But there need to be guardrails and protections in place, because some programs should be quickly dismissed as ineffective — but they aren’t always,” he said.
Carleton’s research found that fewer than 10 mental health programs marketed to Canadian governments — out of 300 in total — are backed up by evidence showing their effectiveness.
In his view, the answer is not complicated — but enormous.
“We’ve got to get way further upstream,” he said.
“We’re rapidly approaching more and more crisis-level challenges… with fewer and fewer [first responders], and we’re asking them to do more and more.”
This article was produced through the Breaking Needles Fellowship Program, which provided a grant to Canadian Affairs, a digital media outlet, to fund journalism exploring addiction and crime in Canada. Articles produced through the Fellowship are co-published by Break The Needle and Canadian Affairs.

From the Fraser Institute
While running for the job of leading the country, Prime Minister Carney promised to defend the Canada Health Act (CHA) and build a health-care system Canadians can be proud of. Unfortunately, to have any hope of accomplishing the latter promise, he must break the former and reform the CHA.
As long as Ottawa upholds and maintains the CHA in its current form, Canadians will not have a timely, accessible and high-quality universal health-care system they can be proud of.
Consider for a moment the remarkably poor state of health care in Canada today. According to international comparisons of universal health-care systems, Canadians endure some of the lowest access to physicians, medical technologies and hospital beds in the developed world, and wait in queues for health care that routinely rank among the longest in the developed world. This is all happening despite Canadians paying for one of the developed world’s most expensive universal-access health-care systems.
None of this is new. Canada’s poor ranking in the availability of services—despite high spending—reaches back at least two decades. And wait times for health care have nearly tripled since the early 1990s. Back then, in 1993, Canadians could expect to wait 9.3 weeks for medical treatment after GP referral compared to 30 weeks in 2024.
But fortunately, we can find the solutions to our health-care woes in other countries such as Germany, Switzerland, the Netherlands and Australia, which all provide more timely access to quality universal care. Every one of these countries requires patient cost-sharing for physician and hospital services, and allows private competition in the delivery of universally accessible services with money following patients to hospitals and surgical clinics. And all these countries allow private purchases of health care, as this reduces the burden on the publicly-funded system and creates a valuable pressure valve for it.
And this brings us back to the CHA, which contains the federal government’s requirements for provincial policymaking. To receive their full federal cash transfers for health care from Ottawa (totalling nearly $55 billion in 2025/26) provinces must abide by CHA rules and regulations.
And therein lies the rub—the CHA expressly disallows requiring patients to share the cost of treatment while the CHA’s often vaguely defined terms and conditions have been used by federal governments to discourage a larger role for the private sector in the delivery of health-care services.
Clearly, it’s time for Ottawa’s approach to reflect a more contemporary understanding of how to structure a truly world-class universal health-care system.
Prime Minister Carney can begin by learning from the federal government’s own welfare reforms in the 1990s, which reduced federal transfers and allowed provinces more flexibility with policymaking. The resulting period of provincial policy innovation reduced welfare dependency and government spending on social assistance (i.e. savings for taxpayers). When Ottawa stepped back and allowed the provinces to vary policy to their unique circumstances, Canadians got improved outcomes for fewer dollars.
We need that same approach for health care today, and it begins with the federal government reforming the CHA to expressly allow provinces the ability to explore alternate policy approaches, while maintaining the foundational principles of universality.
Next, the Carney government should either hold cash transfers for health care constant (in nominal terms), reduce them or eliminate them entirely with a concordant reduction in federal taxes. By reducing (or eliminating) the pool of cash tied to the strings of the CHA, provinces would have greater freedom to pursue reform policies they consider to be in the best interests of their residents without federal intervention.
After more than four decades of effectively mandating failing health policy, it’s high time to remove ambiguity and minimize uncertainty—and the potential for politically motivated interpretations—in the CHA. If Prime Minister Carney wants Canadians to finally have a world-class health-care system then can be proud of, he should allow the provinces to choose their own set of universal health-care policies. The first step is to fix, rather than defend, the 40-year-old legislation holding the provinces back.



RFK Jr. says Hep B vaccine is linked to 1,135% higher autism rate

Alberta Independence Seekers Take First Step: Citizen Initiative Application Approved, Notice of Initiative Petition Issued

RFK Jr. Unloads Disturbing Vaccine Secrets on Tucker—And Surprises Everyone on Trump
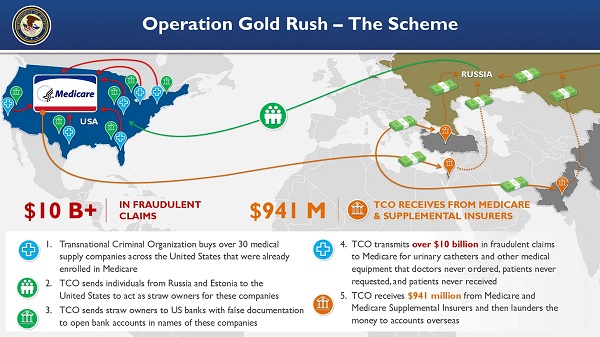
National Health Care Fraud Takedown Results in 324 Defendants Charged in Connection with Over $14.6 Billion in Alleged Fraud
-
 Crime2 days ago
Crime2 days ago“This is a total fucking disaster”
-
 Fraser Institute1 day ago
Fraser Institute1 day agoBefore Trudeau average annual immigration was 617,800. Under Trudeau number skyrocketted to 1.4 million annually
-
 International2 days ago
International2 days agoChicago suburb purchases childhood home of Pope Leo XIV
-
 Daily Caller2 days ago
Daily Caller2 days ago‘I Know How These People Operate’: Fmr CIA Officer Calls BS On FBI’s New Epstein Intel
-
 MAiD2 days ago
MAiD2 days agoCanada’s euthanasia regime is already killing the disabled. It’s about to get worse
-
 Daily Caller2 days ago
Daily Caller2 days agoBlackouts Coming If America Continues With Biden-Era Green Frenzy, Trump Admin Warns
-
 Red Deer2 days ago
Red Deer2 days agoJoin SPARC in spreading kindness by July 14th
-
Business1 day ago
Prime minister can make good on campaign promise by reforming Canada Health Act