Health
Public coverage of cross-border health care would help reduce waiting times

News release from the Montreal Economic Institute and Second Street
450,000 European patients had surgery outside their country of residence in 2022
Allowing Canadian patients to get reimbursed from the government for care received outside the country – just like Europeans do – would help reduce waiting times, according to an economic note published jointly by the Montreal Economic Institute and SecondStreet.org this morning.
“Long waiting times for surgery in Canada have damaging effects on patients‘ health and quality of life,” says Frederik Cyrus Roeder, health economist and author of the study. “Allowing Canadian patients to seek treatment elsewhere would help them regain their health, while breaking the cycle of constant catching up in Canadian healthcare systems.”
Since 2011, European patients have been permitted to seek treatment in any EU member country and receive reimbursement of their medical expenses equivalent to what their national health insurance plan would have covered at home.
This mechanism is known as the “cross-border directive,” or the “patients’ rights directive.”
Thanks to this arrangement, 450,000 European patients were able to access elective surgery outside their country of residence in 2022. Nearly 80% of the requests submitted that year were approved.
The economist explains that a large part of the voluntary program’s success is due to the fact that it acts as a safety valve when healthcare systems are no longer delivering.
“Such a system is no more expensive for the public insurer, because the reimbursements provided cannot exceed the costs of delivering the same treatment in the local healthcare system,” explains Mr. Roeder. “Where this directive really comes into its own is when a healthcare system can no longer manage to treat patients within an acceptable timeframe.”
“Patients are then free to turn to other alternatives without having to pay a stiff price. It’s important to note that even patients who don’t want to travel for treatment still benefit from this as it helps shorten waiting lists.”
In 2023, more than four out of ten Canadian patients had to wait longer than the recommended time to obtain a knee replacement in Canada. For hip replacements, the figure was one in three.
The joint study by the MEI and SecondStreet.org is available here.
* * *
The MEI is an independent public policy think tank with offices in Montreal and Calgary. Through its publications, media appearances, and advisory services to policymakers, the MEI stimulates public policy debate and reforms based on sound economics and entrepreneurship.
SecondStreet.org launched in 2019 to focus on researching how government policies affect everyday Canadians. In addition to policy research, we tell short stories featuring Canadians from coast-to-coast explaining how they’re affected by government policies.


By Adam Zivo
Sweden, the U.K., and Canada all experimented with providing opioids to addicts. The results were disastrous.
[This article was originally published in City Journal, a public policy magazine and website published by the Manhattan Institute for Policy Research. We encourage our readers to subscribe to them for high-quality analysis on urban issues]
Last August, Denver’s city council passed a proclamation endorsing radical “harm reduction” strategies to address the drug crisis. Among these was “safer supply,” the idea that the government should give drug users their drug of choice, for free. Safer supply is a popular idea among drug-reform activists. But other countries have already tested this experiment and seen disastrous results, including more addiction, crime, and overdose deaths. It would be foolish to follow their example.
The safer-supply movement maintains that drug-related overdoses, infections, and deaths are driven by the unpredictability of the black market, where drugs are inconsistently dosed and often adulterated with other toxic substances. With ultra-potent opioids like fentanyl, even minor dosing errors can prove fatal. Drug contaminants, which dealers use to provide a stronger high at a lower cost, can be just as deadly and potentially disfiguring.
Because of this, harm-reduction activists sometimes argue that governments should provide a free supply of unadulterated, “safe” drugs to get users to abandon the dangerous street supply. Or they say that such drugs should be sold in a controlled manner, like alcohol or cannabis—an endorsement of partial or total drug legalization.
But “safe” is a relative term: the drugs championed by these activists include pharmaceutical-grade fentanyl, hydromorphone (an opioid as potent as heroin), and prescription meth. Though less risky than their illicit alternatives, these drugs are still profoundly dangerous.
The theory behind safer supply is not entirely unreasonable, but in every country that has tried it, implementation has led to increased suffering and addiction. In Europe, only Sweden and the U.K. have tested safer supply, both in the 1960s. The Swedish model gave more than 100 addicts nearly unlimited access through their doctors to prescriptions for morphine and amphetamines, with no expectations of supervised consumption. Recipients mostly sold their free drugs on the black market, often through a network of “satellite patients” (addicts who purchased prescribed drugs). This led to an explosion of addiction and public disorder.
Most doctors quickly abandoned the experiment, and it was shut down after just two years and several high-profile overdose deaths, including that of a 17-year-old girl. Media coverage portrayed safer supply as a generational medical scandal and noted that the British, after experiencing similar problems, also abandoned their experiment.
While the U.S. has never formally adopted a safer-supply policy, it experienced something functionally similar during the OxyContin crisis of the 2000s. At the time, access to the powerful opioid was virtually unrestricted in many parts of North America. Addicts turned to pharmacies for an easy fix and often sold or traded their extra pills for a quick buck. Unscrupulous “pill mills” handed out prescriptions like candy, flooding communities with OxyContin and similar narcotics. The result was a devastating opioid epidemic—one that rages to this day, at a cumulative cost of hundreds of thousands of American lives. Canada was similarly affected.
The OxyContin crisis explains why many experienced addiction experts were aghast when Canada greatly expanded access to safer supply in 2020, following a four-year pilot project. They worried that the mistakes of the recent past were being made all over again, and that the recently vanquished pill mills had returned under the cloak of “harm reduction.”
Subscribe for free to get BTN’s latest news and analysis – or donate to our investigative journalism fund.
Most Canadian safer-supply prescribers dispense large quantities of hydromorphone with little to no supervised consumption. Patients can receive up to 40 eight-milligram pills per day—despite the fact that just two or three are enough to cause an overdose in someone without opioid tolerance. Some prescribers also provide supplementary fentanyl, oxycodone, or stimulants.
Unfortunately, many safer-supply patients sell or trade a significant portion of these drugs—primarily hydromorphone—in order to purchase more potent illicit substances, such as street fentanyl.
The problems with safer supply entered Canada’s consciousness in mid-2023, through an investigative report I wrote for the National Post. I interviewed 14 addiction physicians from across the country, who testified that safer-supply diversion is ubiquitous; that the street price of hydromorphone collapsed by up to 95 percent in communities where safer supply is available; that youth are consuming and becoming addicted to diverted safer-supply drugs; and that organized crime traffics these drugs.
Facing pushback, I interviewed former drug users, who estimated that roughly 80 percent of the safer-supply drugs flowing through their social circles was getting diverted. I documented dozens of examples of safer-supply trafficking online, representing tens of thousands of pills. I spoke with youth who had developed addictions from diverted safer supply and adults who had purchased thousands of such pills.
After months of public queries, the police department of London, Ontario—where safer supply was first piloted—revealed last summer that annual hydromorphone seizures rose over 3,000 percent between 2019 and 2023. The department later held a press conference warning that gangs clearly traffic safer supply. The police departments of two nearby midsize cities also saw their post-2019 hydromorphone seizures increase more than 1,000 percent.
The Canadian government quietly dropped its support for safer supply last year, cutting funding for many of its pilot programs. The province of British Columbia (the nexus of the harm-reduction movement) finally pulled back support last month, after a leaked presentation confirmed that safer-supply drugs are getting sold internationally and that the government is investigating 60 pharmacies for paying kickbacks to safer-supply patients. For now, all safer-supply drugs dispensed within the province must be consumed under supervision.
Harm-reduction activists have insisted that no hard evidence exists of widespread diversion of safer-supply drugs, but this is only because they refuse to study the issue. Most “studies” supporting safer supply are produced by ideologically driven activist-scholars, who tend to interview a small number of program enrollees. These activists also reject attempts to track diversion as “stigmatizing.”
The experiences of Sweden, the United Kingdom, and Canada offer a clear warning: safer supply is a reliably harmful policy. The outcomes speak for themselves—rising addiction, diversion, and little evidence of long-term benefit.
As the debate unfolds in the United States, policymakers would do well to learn from these failures. Americans should not be made to endure the consequences of a policy already discredited abroad simply because progressive leaders choose to ignore the record. The question now is whether we will repeat others’ mistakes—or chart a more responsible course.
Our content is always free –
but if you want to help us commission more high-quality journalism,
consider getting a voluntary paid subscription.
Health
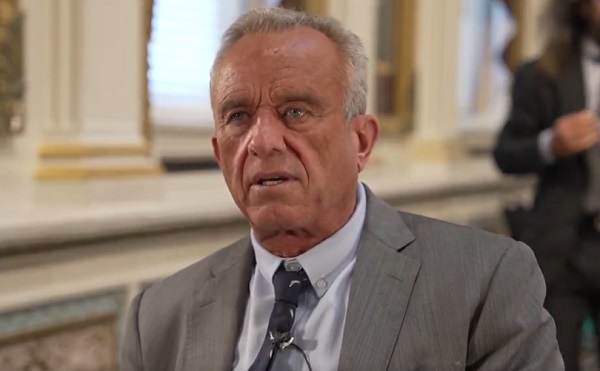
RFK Jr. says ‘everything is going to change’ with CDC vaccine policy in Michael Knowles interview
From LifeSiteNews
New Health and Human Services Director Robert F. Kennedy Jr. said the CDC’s own reporting system ‘captures fewer than 1% of vaccine injuries. It’s worthless, and everybody agrees it’s worthless.’
When Michael Knowles asked new Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. if anything will change regarding the public’s justifiable concern with the growth of vaccines, Kennedy quickly shot back, “Everything is going to change.”
Kennedy pointed to the Centers for Disease Control’s current flawed VAERS (Vaccine Adverse Event Reporting System) online mechanism.
By way of example, he said, “None of the vaccines that are given during the first six months of life have ever been tested for autism. The only one was the DTP vaccine. And that one study that was done, according to the Institute of Medicine, the National Academy of Sciences, found that there was a link.”
But “They threw out that study because it was based upon CDC’s surveillance system, VAERS, and they said that system is no good.”
“That begs the question, why doesn’t CDC have a functional surveillance system?” he asked. “We’re gonna make sure they do.”
“They don’t do pre-licensing safety testing for vaccines” he continued. “They’re the only product that’s exempt. So what they say is, if there are injuries, we’ll capture them afterward.”
However, “they have a system that doesn’t capture them. In fact, CDC’s own study of its own system said it captures fewer than 1% of vaccine injuries,” Kennedy said. “It’s worthless, and everybody agrees it’s worthless.”
“Why have we gone for 39 years and nobody’s fixed it?” he wondered, promising, “We’re gonna fix it.”
“We have DOGE (which) knows how to manage data. We’re going to be able to get into these databases and give answers to the American public,” Kennedy predicted.
“We’re going to have gold standard science, we’re going to follow the science, we’re going to publish all of our datasets, which CDC has never done,” he said.
“We’re going to do replication of all of our studies, which CDC has never done. We’re going to publish our peer review, which CDC has never done,” Kennedy vowed. “So people are going to have real answers for the first time.”
The new HHS head also discussed more broadly his mission after taking over the department’s helm, the mess created by the Biden administration, his job’s challenges, and recent developments thanks to DOGE.
“HHS is a $1.9 trillion agency. It’s the biggest agency in the government. And during the Biden administration, President Biden increased its budget by 38% and increased the workforce by 17%.”
“And by every metric by which we measure public health, health accelerated its decline.”
“When I came to HHS, what I found was a sprawling bureaucracy,” with functional duplication of departments, rampant redundancy and overstaffing, with various sub-agencies often acting in a territorial, self-protecting manner rather than a synergistic one.
“Perverse incentives” sometimes drive employee’s work,” he noted.
Despite his short tenure at HHS, with the help of DOGE, Kennedy has already released 20,000 “bureaucrats” from the department’s ranks.
“We’re going from 82,000 personnel to 62,000,” said Kennedy, carefully pointing out, “We’re keeping the scientists and frontline providers.”
Kennedy said that it has been really hard to fight against the problems at HHS and NIH over the last 40 years from “the outside.”
But “now I’m on the inside,” he declared. “This is the purpose of my life. It’s what I’m going to do over the next four years.”
He concluded:
President Trump promised to return the American dream to Americans.
A healthy person has a thousand dreams. A sick person only has one.


28 energy leaders call for eliminating ALL energy subsidies—even ones they benefit from

Europe Can’t Survive Without America
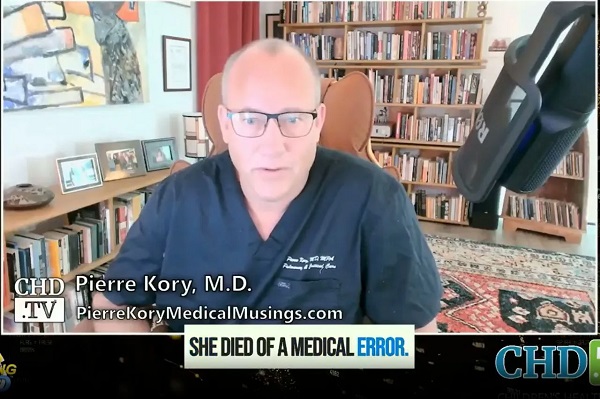
Dr. Pierre Kory Exposes the Truth About the Texas ‘Measles Death’ Hoax

Support For National Pipelines And LNG Projects Gain Momentum, Even In Quebec

-
 Addictions2 days ago
Addictions2 days agoShould fentanyl dealers face manslaughter charges for fatal overdoses?
-
 Also Interesting2 days ago
Also Interesting2 days agoThe bizarre story of Taro Tsujimoto
-
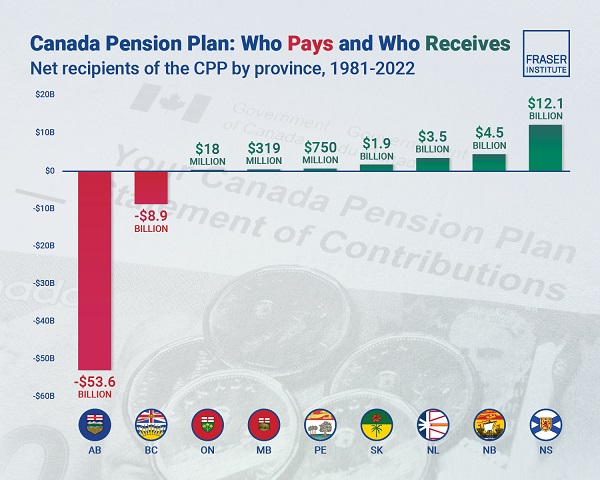 Alberta2 days ago
Alberta2 days agoAlbertans have contributed $53.6 billion to the retirement of Canadians in other provinces
-
 Energy2 days ago
Energy2 days agoEnergy, climate, and economics — A smarter path for Canada
-
 2025 Federal Election2 days ago
2025 Federal Election2 days agoChinese Gangs Dominate Canada: Why Will Voters Give Liberals Another Term?
-
 Health1 day ago
Health1 day agoRFK Jr. Drops Stunning Vaccine Announcement
-
 2025 Federal Election1 day ago
2025 Federal Election1 day agoSoaked, Angry, and Awake: What We Saw at Pierre Poilievre’s Surrey Rally
-
 Energy2 days ago
Energy2 days agoPoll: Majority says energy independence more important than fighting climate change